
Rethinking the Pill in Perimenopause: Why Menopause Hormone Therapy May Be a Better Fit
Written and edited by Sarah Bonza MD, MPH, MSCP, FAAFP, DipABLM, NBC-HWC

As a physician who works closely with women in perimenopause, I hear this question often: “Should I stay on the pill, or is it time to switch to hormone therapy?”
It’s a good question—because perimenopause is a hormonal roller coaster. Estrogen levels spike and crash unpredictably. Ovulation becomes hit-or-miss. And progesterone—the calming, balancing hormone—often fades into the background. The result? Heavy periods, anxiety, insomnia, mood swings, and that unsettling feeling that your body has changed and no one warned you.
For years, the go-to solution has been oral contraceptives. And in certain situations, they can help—especially when contraception is still a must. But in many cases, we now have better tools. Tools that don't just suppress your symptoms, but support your body’s natural rhythms.
At Bonza Health, I often guide women through a more physiologic and personalized approach: menopause hormone therapy (MHT). Especially when we use bioidentical estrogen and progesterone in a cyclical pattern to mimic the luteal phase, MHT can bring symptom relief without overriding your endocrine system. It’s a gentler, more sustainable way to navigate the hormonal chaos of perimenopause—and it aligns with your body, not against it.
Let’s take a closer look at why the pill has been the default for so long—and why it may be time to rethink that default.
The Conventional Approach: Birth Control Pills in Perimenopause
For decades, combined oral contraceptives (COCs) have been the standard prescription for women in their 40s who are experiencing the telltale signs of perimenopause: heavy, unpredictable periods, hot flashes, mood swings, and the occasional "Am I pregnant or just late?" moment.
These pills serve a few key roles:
They regulate erratic bleeding, offering predictable cycles.
They can blunt vasomotor symptoms like hot flashes and night sweats.
And most importantly, they provide reliable contraception—something that still matters, as many women remain ovulatory into their late 40s and early 50s.
Professional organizations like the North American Menopause Society (NAMS) and the American College of Obstetricians and Gynecologists (ACOG) support the use of low-dose COCs in healthy, non-smoking women under 50–55 who still need birth control and symptom relief. In the right context, they can be effective.
But here’s the catch—and it’s an important one: oral contraceptives suppress your body’s natural hormone production. They override your own rhythm with synthetic hormones, typically ethinyl estradiol and progestins like levonorgestrel. These are not bioidentical. They’re delivered at doses higher than what’s needed just to manage perimenopausal symptoms—because their primary goal is to shut down ovulation and prevent pregnancy.
While that may be appropriate in some cases, it can also mask the transition into menopause, and for many women, it exacerbates other issues like mood instability, breast tenderness, or weight gain. In essence, the pill was designed for a younger body with different priorities—and it doesn’t always serve a woman in midlife with the same nuance or gentleness that we now know is possible.
That’s where hormone therapy—done right—comes in.
The Functional & Naturopathic Perspective: Hormonal Support, Not Suppression
At Bonza Health, we approach perimenopause not as a medical problem to be fixed, but as a natural—and often transformative—transition. It’s a time when your hormones are recalibrating, and your body is asking for support, not suppression.
From a functional and naturopathic lens, the goal isn’t to override your hormonal rhythms with high-dose synthetic hormones. It’s to work with your body’s existing fluctuations, gently smoothing the peaks and valleys so you can feel like yourself again.
Here’s what that looks like in practice:
Cycle Tracking: Instead of silencing your cycle, we pay attention to it. Tracking patterns helps us understand where you are hormonally—and what your body is trying to tell us.
Adrenal and Thyroid Support: As ovarian hormone production becomes more erratic, your adrenals and thyroid often pick up the slack. When those systems are overburdened—hello, fatigue, anxiety, and weight changes—we focus on restoring balance and resilience.
Cyclical Bioidentical Hormone Therapy: Rather than using a one-size-fits-all pill, we support your natural rhythm with low-dose bioidentical estradiol and progesterone, timed to mimic your luteal phase. This can stabilize mood, improve sleep, ease breast tenderness, and help you feel grounded—even in the hormonal storm.
Nutritional and Botanical Support: We may use evidence-based compounds like DIM (diindolylmethane) and calcium-D-glucarate to assist estrogen metabolism and clearance, reducing symptoms of estrogen dominance like bloating, heavy bleeding, and irritability.
This approach aligns beautifully with the core principles of Lifestyle Medicine and functional medicine: use the lowest effective dose of the most natural intervention, and address the root causes—not just the symptoms.
Perimenopause isn’t a disease. It’s a rite of passage. And when we treat it with respect and intention, we give women the opportunity not just to survive it—but to emerge stronger, more self-aware, and more in control of their health than ever before.

The Case for Menopause Hormone Therapy (MHT) in Perimenopause
When women in their 40s come to me exhausted, anxious, and overwhelmed by unpredictable periods and mood swings, they often feel like they’re falling apart. But what’s really happening is a hormonal shift—and when we support that shift with the right tools, everything can start to feel manageable again.
That’s where menopause hormone therapy (MHT) comes in. And no, it’s not just for women who’ve already gone a full year without a period. Used thoughtfully, MHT can be incredibly effective during perimenopause, especially when we use it to mirror the body’s natural rhythm.
Modern MHT typically involves two key components:
Bioidentical estradiol—usually delivered transdermally through a patch, gel, or spray. This mimics the estrogen your ovaries used to make and avoids the liver metabolism associated with oral estrogen, offering a safer metabolic profile.
Micronized progesterone—either as a capsule (like Prometrium®) or compounded cream or lozenge. This is bioidentical and generally better tolerated than synthetic progestins.
One of the most powerful strategies we use is cyclical hormone therapy: giving estradiol consistently and adding progesterone only during the luteal phase (typically days 14–28). This approach mimics the way your body would naturally produce hormones if you were still ovulating regularly.
The benefits:
Stabilizes mood, sleep, and anxiety by smoothing out hormonal peaks and valleys.
Preserves endogenous hormone production instead of shutting it down entirely.
May still allow for ovulation, which helps maintain adrenal function, insulin sensitivity, and long-term endocrine health.
Supports metabolism and cardiovascular health, particularly when transdermal estrogen is used (which doesn’t increase clot risk the way oral estrogen or birth control pills can).
And importantly—it’s customizable. Doses can be adjusted based on your symptoms, lab work, and goals.
Instead of suppressing your hormonal landscape, MHT can support and strengthen it. And when it's done right—personalized, physiologic, and rooted in your unique needs—it becomes a powerful way to reclaim calm, clarity, and vitality during the most hormonally turbulent decade of a woman’s life.
Comparing the Two Approaches
When women ask me whether they should stay on the Pill or consider hormone therapy, I walk them through this side-by-side comparison. While both options involve hormones, they’re fundamentally different in purpose, formulation, and how they interact with your body.
Let’s break it down:
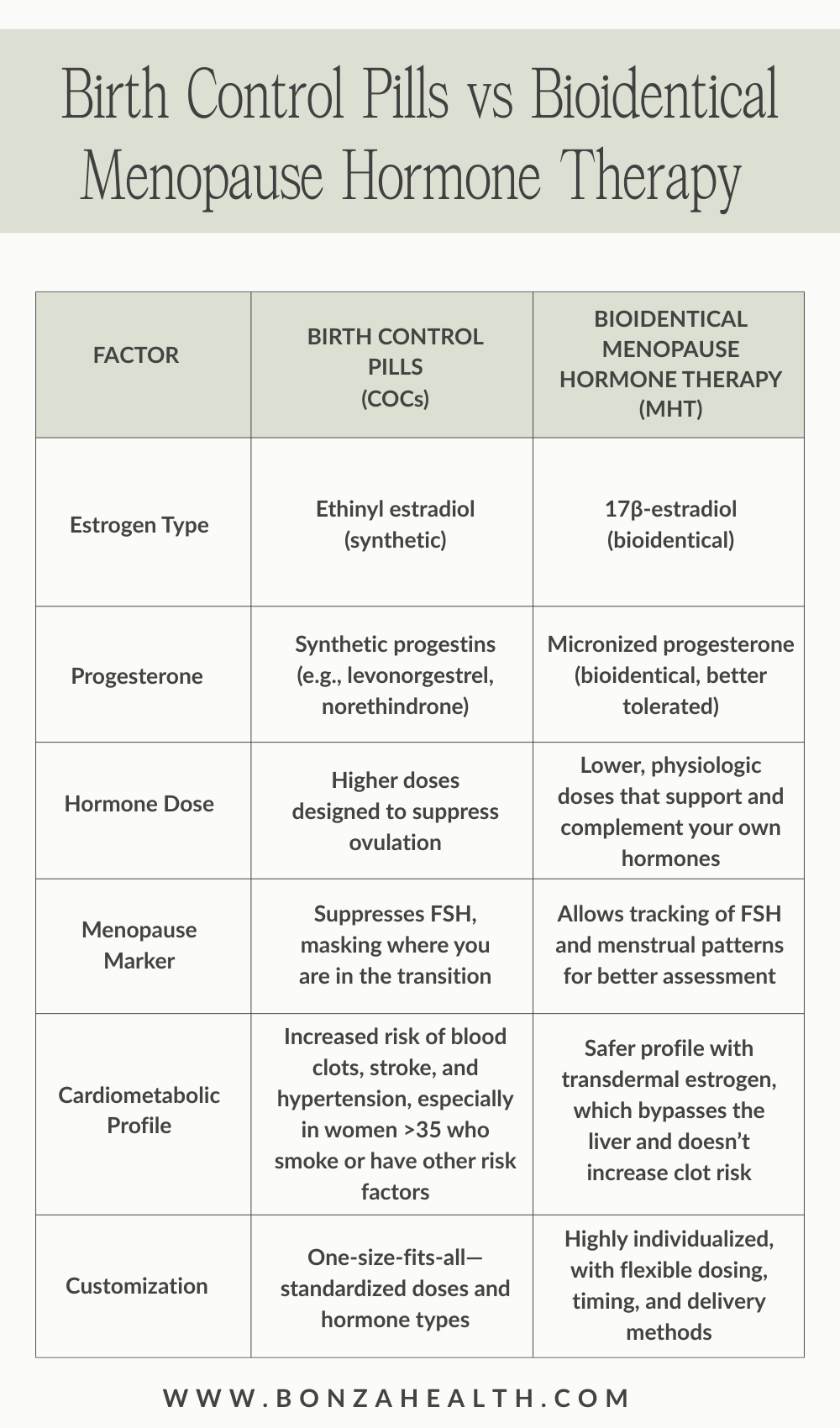
The Pill was designed for a different life stage—primarily to prevent pregnancy. Menopause hormone therapy, on the other hand, was created to support hormonal health during the midlife transition, not suppress it. When we choose bioidentical MHT, especially in a cyclic pattern, we’re working with your body, not against it.
Expert Recommendations (With a Nuanced Lens)
According to the North American Menopause Society (NAMS) 2022 Position Statement, combined oral contraceptives (COCs) are considered appropriate for symptom relief and contraception in healthy, non-smoking women under age 50. They can help manage irregular bleeding, hot flashes, and perimenopausal mood swings—especially when birth control is still needed.
But here’s the nuance: while the statement favors transitioning to menopause hormone therapy (MHT) after menopause, it doesn’t exclude using MHT earlier—during perimenopause—particularly when contraception is no longer a primary concern.
In fact, for many women in their mid-to-late 40s, the benefits of MHT can outweigh those of the Pill, especially when the goal is symptom control, not pregnancy prevention.
What’s more, modern MHT—using transdermal estradiol paired with micronized progesterone—has a strong safety profile. This combination is considered low-risk even in women with certain comorbidities, such as:
Migraines without aura
Mild hypertension
Metabolic syndrome or insulin resistance
Because transdermal estrogen bypasses the liver, it avoids the increased risk of blood clots associated with oral estrogens and ethinyl estradiol found in the Pill. And micronized progesterone, a bioidentical option, is better tolerated and may even have neuroprotective and sleep-supportive effects.
The key is individualization. Expert guidelines provide the foundation, but your care should be tailored to your symptoms, your risks, and your goals.
At Bonza Health, we use these recommendations as a compass—not a cage. That allows us to blend science, safety, and personalization to help you feel better now—without waiting for full-blown menopause to arrive.
When to Prefer MHT Over COCs
There are times when oral contraceptives make sense—especially if reliable birth control is still a top priority. But for many women in perimenopause, symptom relief—not contraception—is the main goal. And in those cases, menopause hormone therapy (MHT) often offers a more effective, gentle, and personalized solution.
Here’s when I recommend considering MHT over COCs:
When mood swings, poor sleep, anxiety, or breast tenderness are peaking mid-cycle—often a sign of hormonal imbalance, not just cycle irregularity.
When heavy bleeding and fatigue are driven by estrogen dominance—a state where estrogen is high and unopposed by adequate progesterone. Suppressing the cycle with synthetic hormones may not address the root cause, but cycling bioidentical progesterone can.
When synthetic progestins aren't well tolerated. Some women experience worsening mood, bloating, or even depression on the Pill. Switching to micronized, bioidentical progesterone often brings welcome relief.
When a woman wants a more natural, intuitive approach—one that respects her body’s signals instead of silencing them. MHT allows for hormone tracking, dose adjustments, and an aligned sense of well-being many women don’t feel on the Pill.

One especially powerful approach is cycling bioidentical hormones in the luteal phase—typically days 14–28 of the cycle. This mimics the body’s natural hormone rhythm and addresses relative progesterone insufficiency, which is common in perimenopause and often responsible for mid-cycle anxiety, insomnia, and breast tenderness. Supporting progesterone during this window helps stabilize estrogen peaks, calm the nervous system, and ease the emotional turbulence many women describe as “I just don’t feel like myself anymore.”
In these cases, MHT isn’t just a replacement for the Pill—it’s a more physiologic, empowering step toward hormonal harmony.
Conclusion
While combined oral contraceptives (COCs) can be helpful for contraception—and occasionally symptom control—they may not be the most appropriate hormonal support for women navigating the emotional, metabolic, and cognitive shifts of perimenopause. These years are marked by complexity: unpredictable cycles, estrogen dominance, progesterone deficiency, and the profound impact of hormonal fluctuations on mood, sleep, and overall well-being.
Rather than override these rhythms with synthetic hormones designed for a younger body, we now have the tools to support them—with greater precision and compassion.
Menopause hormone therapy (MHT), especially when bioidentical and cycled in alignment with the luteal phase, offers a more physiologic, individualized, and sustainable path forward. It respects your body’s natural transitions, supports long-term health, and allows you to feel like yourself again—calm, clear, and in control.
As our understanding of women’s health evolves, so should our approach. It's time to move beyond the outdated reflex of prescribing the Pill and embrace the nuanced, evidence-informed strategies that truly meet women where they are.
Because midlife isn’t the beginning of the end—it’s the beginning of your better. And you deserve care that reflects that.
