
Body Composition Changes During Perimenopause and Menopause: A Comprehensive Guide
Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Understanding how your body changes during menopause is important for prolonging your healthspan
The menopausal transition represents a significant period of physiological change for women, with profound effects on body composition, metabolism, and overall health. Understanding these changes is crucial for implementing effective strategies to maintain health and vitality during this transition. This comprehensive examination explores how women's bodies change for better or worse, during perimenopause and menopause, the underlying mechanisms driving these changes, and evidence-based approaches to mitigate negative health outcomes.
The Evolution of Body Composition During the Menopausal Transition
The perimenopause and menopause transitions brings distinct and measurable changes to women's body composition. Research has confirmed that during a typical 3.5-year menopause transition—approximately two years before the final menstrual period and 1.5 years after—women experience an average weight gain of about 3.5 pounds (1.6 kg), representing a 6% increase in body weight. [1]. Simultaneously, there is a decrease in lean mass, albeit less dramatic than weight gain, with women losing an average of 0.4 pounds (0.2 kg) of muscle, or about 0.5% of muscle mass during this period [1].
The rate of fat gain essentially doubles from the time period prior to menopause once the transition begins [1]. These changes don't occur uniformly throughout the body but instead follow a predictable pattern of redistribution. While premenopausal women typically store fat in the hips and thighs (gynoid distribution), the menopausal transition shifts fat storage toward the abdomen (android distribution) [5]. This is evidenced by a significantly lower android-to-gynoid ratio in premenopausal women compared to perimenopausal women.
What's particularly noteworthy is the timing of these changes. The Study of Women's Health Across the Nation (SWAN) found that fat and lean mass increased prior to the menopause transition, but at the start of the transition, the rate of fat gain doubled while lean mass began to decline [13]. These gains and losses continue until approximately two years after the final menstrual period, after which the trajectories of fat and lean mass decelerated to a plateau [13].
Understanding Visceral vs. Subcutaneous Fat Distribution
The distinction between visceral and subcutaneous fat is crucial for understanding the health implications of menopausal body composition changes. Subcutaneous fat lies just beneath the skin and can be felt when pinching excess tissue around the midsection [20]. While all women gain subcutaneous abdominal fat (SAT) with age, only those going through menopause experience a significant increase in visceral adipose tissue (VAT) [6].
Visceral fat accumulates deep within the abdomen, surrounding internal organs [20]. This type of fat is metabolically active and produces inflammatory compounds and hormones that significantly increase health risks. A cross-sectional study of 33 women between 45 and 60 years found that menopause was associated with adipocyte hypertrophy (enlarged fat cells), increased inflammation, hypoxia, and fibrosis in both subcutaneous and visceral adipose tissue [2]. Most concerning, these postmenopausal changes in visceral adipose tissue were specifically associated with decreased insulin sensitivity [2].
The Hormonal Mechanisms Behind Body Composition Changes
The primary driver behind these body composition changes is the dramatic decline in estrogen that characterizes menopause. Estrogen plays a multifaceted role in regulating body fat distribution, energy metabolism, and insulin sensitivity in women [16]. As estrogen levels fall during the menopause transition, the body becomes less responsive to insulin, predisposing women to insulin resistance [3].
A new meta-analysis of 17 different randomized, controlled trials covering more than 29,000 participants found that hormone therapy significantly reduced insulin resistance in healthy postmenopausal women [3]. This provides compelling evidence for estrogen's role in maintaining insulin sensitivity. When estrogen is lost during menopause, elevated blood sugar that cannot enter muscle cells is converted to fat and stored, particularly in the abdominal region [15].
The hormonal landscape becomes further complicated as the balance shifts. With decreased estrogen, the relative influence of testosterone increases, which contributes to the central adiposity pattern characteristic of post-menopausal women [10]. This hormonal reconfiguration also affects energy expenditure—menopause onset is associated with decreased energy expenditure and fat oxidation, creating a metabolic environment conducive to weight gain if lifestyle adjustments aren't made [6].
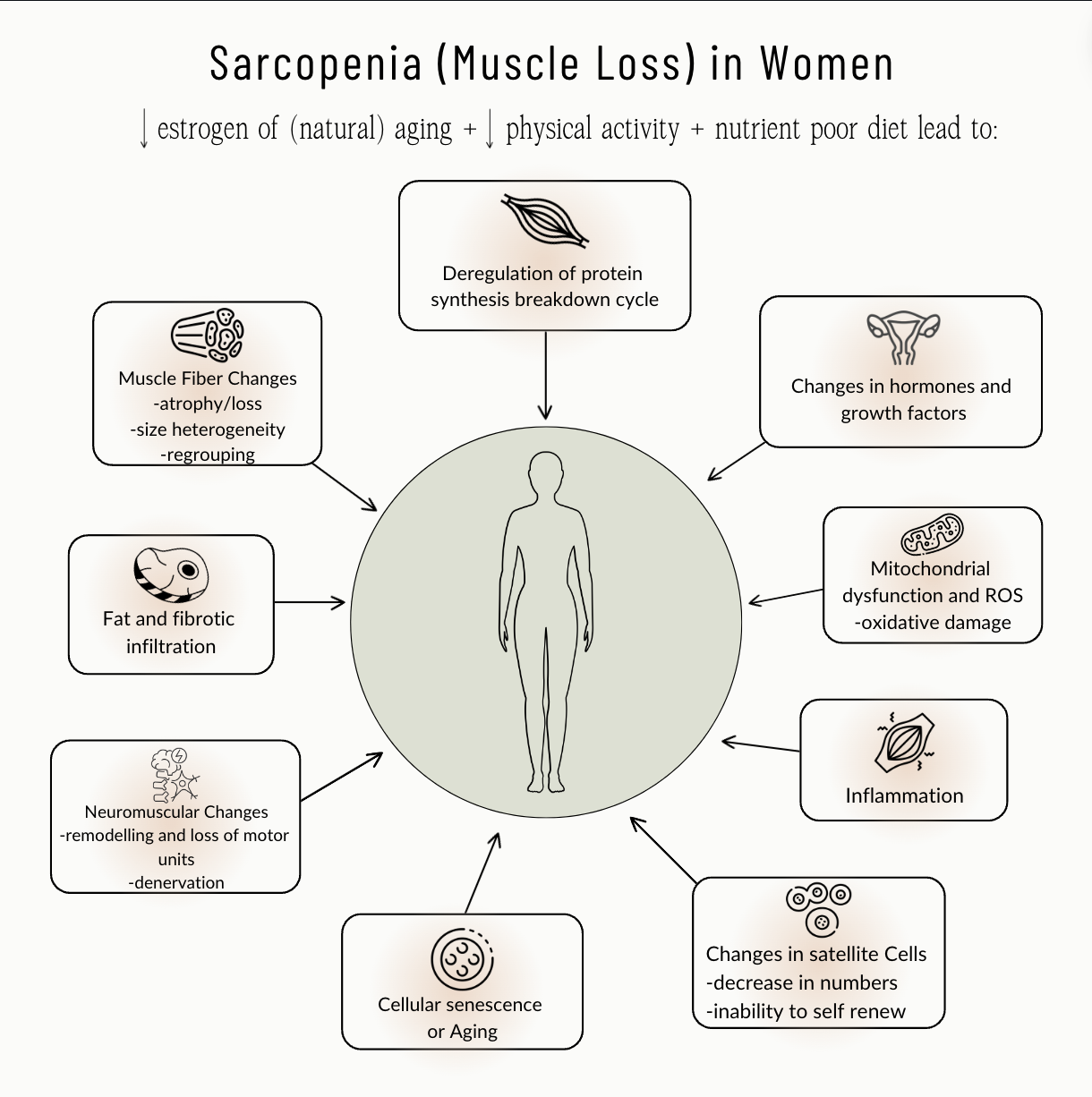
Sarcopenia and Bone Health: The Impact of Estrogen Decline
Beyond changes in fat distribution, the decline in estrogen significantly affects muscle and bone health. Sarcopenia—the progressive loss of muscle mass, strength, and function—is a common condition in post-menopausal women that can result in falls, fractures, physical disability, and even premature death [1,8].
Estradiol, the most potent form of estrogen, has beneficial effects on skeletal muscle by stimulating satellite cell proliferation—the stem cells responsible for muscle regeneration and growth [4]. Research has demonstrated that skeletal muscle contains specific receptors for estradiol, allowing muscle fibers to respond directly to hormonal control [4]. Additionally, estradiol helps limit inflammatory stress damage on skeletal muscle, providing another protective mechanism that diminishes during menopause [4].
The relationship between estrogen and bone health is equally significant. Decreased estrogen levels are closely linked with increased bone resorption, leading to a higher risk of osteoporosis [12]. The combination of decreased muscle mass (sarcopenia) and reduced bone density (osteopenia/osteoporosis) creates a concerning scenario that increases the risk of falls and fractures in postmenopausal women [12].
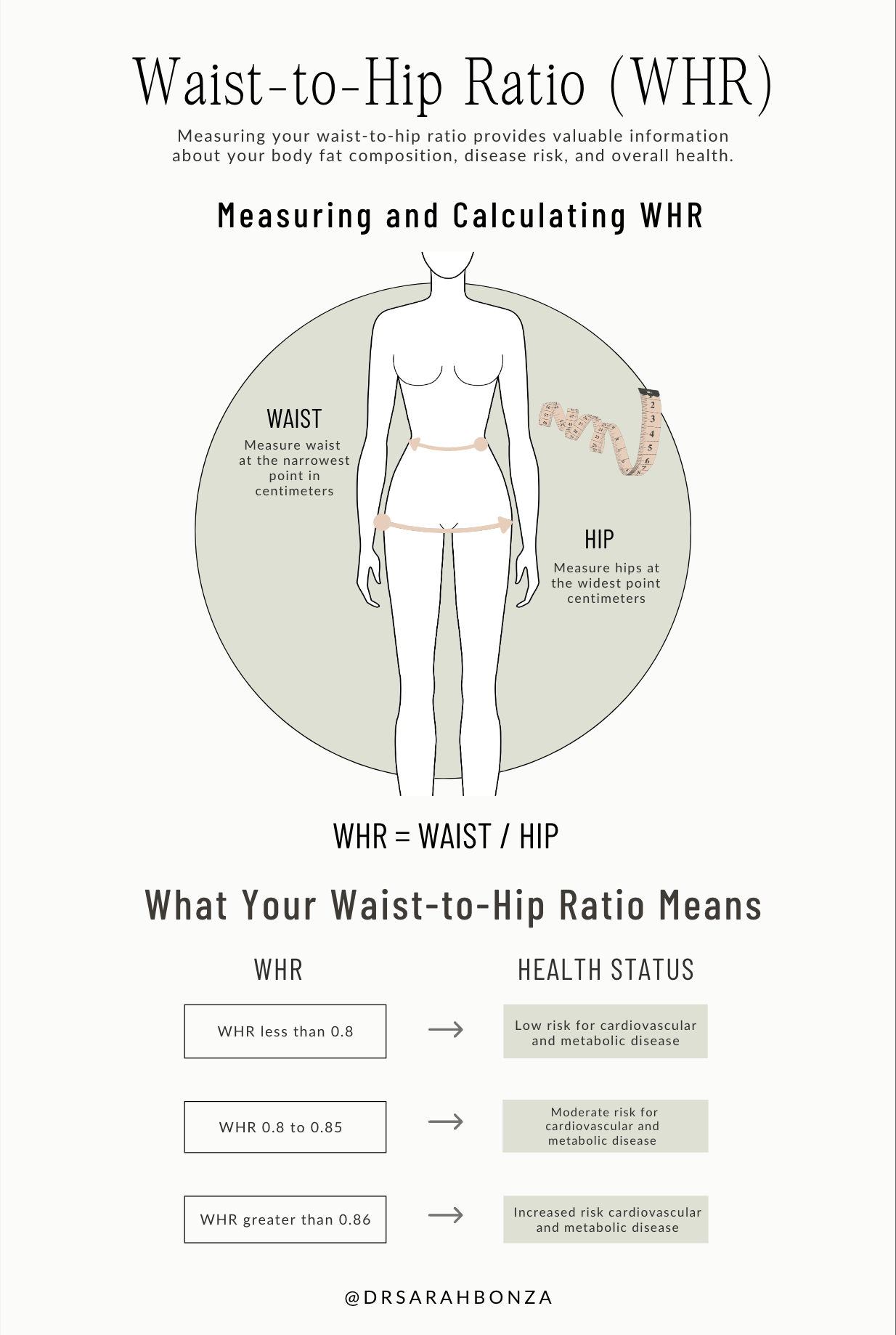
Waist-to-Hip Ratio as a Critical Health Indicator
The shift in fat distribution during menopause makes waist-to-hip ratio (WHR) an especially important health metric for menopausal women. Research indicates that the android-to-gynoid ratio (a measure similar to WHR) is significantly lower in premenopausal than perimenopausal women [5]. This ratio isn't merely an aesthetic concern—it's a powerful predictor of health outcomes.
An elevated waist-to-hip ratio indicates predominant abdominal fat storage, which is associated with increased risk for cardiovascular disease, type 2 diabetes, and certain cancers [20]. Even when women maintain a normal body mass index (BMI), a large waistline increases the risk of dying from cardiovascular disease [20]. This makes WHR a more informative measurement than weight alone for assessing health risks during and after menopause.
Perimenopause: The Critical Window for Intervention
One of the most important findings from recent research is that perimenopause represents a critical window for intervention. Studies show that the greatest changes in overall percentage of body fat occur between premenopause and perimenopause, with these changes later stabilizing in postmenopause [9]. This suggests that initiating lifestyle changes during perimenopause may be most effective in preventing adverse body composition outcomes [5].
As noted by researchers at the University of North Carolina, lifestyle intervention may be most effective in perimenopause, as women experience the onset of poor body composition and metabolism associated with menopause [5]. The perimenopause period provides a unique opportunity to implement preventive strategies before negative body composition changes become established and more difficult to reverse.
The Six Pillars of Lifestyle Medicine for Menopausal Health
Addressing the complex body composition changes of menopause requires a comprehensive approach. The six pillars of lifestyle medicine provide an evidence-based framework:

1. Nutrition
A vibrant and nutritious diet rich in complex carbohydrates, lean proteins, and healthy fats (nuts, seeds, avocados, olive/avocado oils) can help lower inflammation and support metabolic health during menopause [14]. Focusing on nutrient-dense whole foods helps manage insulin resistance, which becomes more prominent with declining estrogen levels.
2. Physical Activity
Regular physical activity is crucial as muscle mass naturally decreases with age. Both aerobic exercise and resistance training are important—the former for cardiovascular health and the latter for preserving muscle mass and bone density [17]. Research shows that physical activity significantly decreases about two years before menopause and remains low thereafter, highlighting the need for conscious efforts to maintain activity levels [6].
3. Stress Management
Stress elevates cortisol levels, which can exacerbate abdominal fat storage. During perimenopause and menopause, women have a higher risk of mood changes, especially those with prior history of anxiety, depression, or premenstrual syndrome [18]. Implementing effective stress management techniques such as mindfulness meditation, yoga, or other relaxation practices can help mitigate these effects.
4. Sleep
Sleep disruption is common during perimenopause and menopause, often due to night sweats and hormonal fluctuations. Poor sleep affects hunger hormones—decreasing leptin (a natural appetite suppressant) and increasing ghrelin (which signals hunger) [18]. Prioritizing sleep hygiene becomes especially important during this transition to prevent weight gain associated with sleep deprivation.
5. Avoidance of Risky Substances
Excessive alcohol consumption and smoking can exacerbate menopausal symptoms and accelerate bone loss. Reducing or eliminating these substances supports overall health and improves body composition outcomes during menopause.
6. Social Connection
Social support and connection contribute significantly to overall well-being and can help women navigate the psychological and physical challenges of menopause. Strong social networks provide motivation for maintaining healthy behaviors and emotional resilience during this transition.
Hormone Therapy Considerations
Beyond lifestyle interventions, hormone therapy (HT) merits consideration for managing both menopausal symptoms and metabolic health. The meta-analysis presented at the 2024 Annual Meeting of The Menopause Society found that hormone therapy—including estrogen alone or estrogen plus progestogen, administered through both oral and transdermal routes—significantly reduced insulin resistance in healthy postmenopausal women [3,7].
While individual health factors must be considered when deciding on hormone therapy, this research suggests that HT may offer metabolic benefits beyond symptom relief. Dr. Stephanie Faubion, medical director for The Menopause Society, noted that "This new meta-analysis is important as declining estrogen levels in menopausal women put them at greater risk for insulin resistance and hormone therapy could be beneficial in reducing insulin resistance in these women" [7].
Conclusion
The menopausal transition brings significant changes to women's body composition, with far-reaching implications for long-term health. Understanding the science behind these changes—from hormonal mechanisms to their effects on fat distribution, muscle mass, and bone density—provides the foundation for proactive health management during this critical life stage.
The evidence clearly shows that perimenopause represents a vital window for intervention, offering women the opportunity to implement lifestyle changes before adverse body composition changes become established. By embracing the six pillars of lifestyle medicine and considering appropriate medical interventions like hormone therapy, women can navigate this transition with greater control over their health outcomes.
Rather than viewing menopausal body composition changes as inevitable, women can approach this phase armed with knowledge and evidence-based strategies to maintain their vitality, strength, and metabolic health for decades to come.

Sign up for Fullscript to shop professional-grade perimenopause supplements.