
It's Not Just Aging: The Hidden Connection Between Estrogen and Your Rising Cholesterol
Written and edited by Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Declining estrogen levels fundamentally alter how the body processes cholesterol
If you're a woman approaching or past menopause, you've likely experienced a familiar scenario at the doctor's office. Your annual bloodwork comes back, and suddenly your cholesterol numbers are creeping upward. Your physician shrugs and says, "It's just part of getting older. We may need to consider a statin." But what if there's more to the story? What if the dramatic hormonal shifts happening in your body are directly influencing those lipid numbers—and what if addressing the root cause could make a meaningful difference?
The relationship between estradiol (the primary form of estrogen in the female body) and cholesterol metabolism is well-established in the medical literature, yet it remains one of the most overlooked factors in women's cardiovascular health. Research published in peer-reviewed journals consistently demonstrates that declining estrogen levels fundamentally alter how the body processes cholesterol. Understanding this connection can empower you to have more informed conversations with your healthcare provider and advocate for your cardiovascular health.
The Menopause-Cholesterol Connection: What the Research Shows
The scientific evidence is clear and compelling. A study published in the Journal of Clinical and Diagnostic Research compared premenopausal and postmenopausal women and found statistically significant increases in total cholesterol, triglycerides, LDL cholesterol (the "bad" cholesterol), and VLDL cholesterol after menopause. Meanwhile, HDL cholesterol (the "good" cholesterol) showed significant decreases. The researchers specifically identified reduced estrogen concentrations as the mechanism driving these changes [1].
This isn't an isolated finding. Research from the Study of Women's Health Across the Nation (SWAN) tracked women longitudinally through the menopausal transition and documented that increases in LDL cholesterol and triglycerides, along with declines in HDL cholesterol, were greater during perimenopause than during the postmenopausal years [2]. This timing is crucial—the lipid changes begin during the transition, often before a woman has even realized she's entering menopause.
A comparative study published in Maturitas found that postmenopausal women had significantly increased total cholesterol (10%), LDL cholesterol (14%), and apolipoprotein B (8.2%) compared to age-matched premenopausal women. The researchers concluded that these are "the primary cardiovascular risk factors affected by menopause"—not simply aging alone [3].
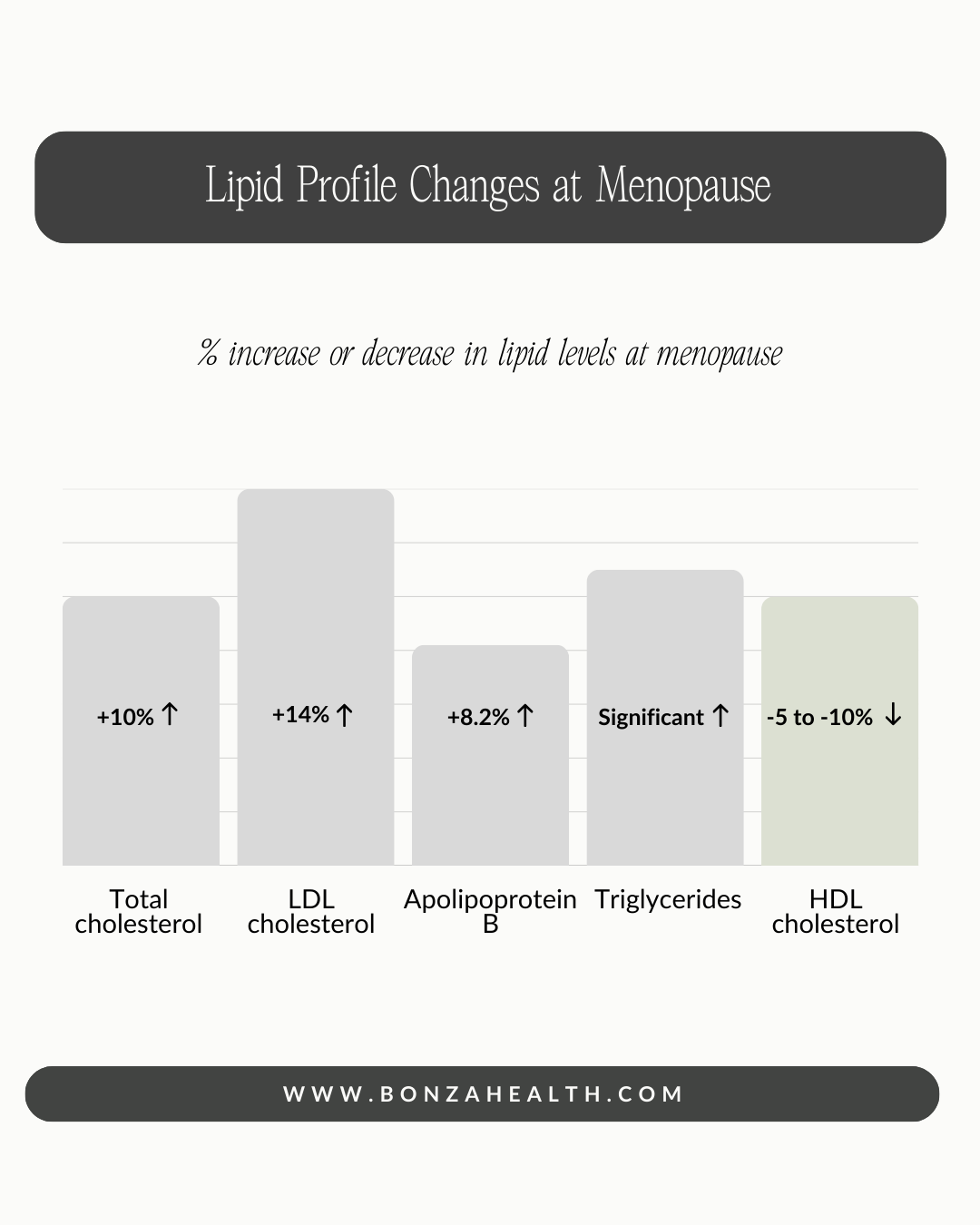
Changes in lipid profiles at menopause
How Estrogen Protects Your Cardiovascular System
Estradiol isn't just a reproductive hormone—it's a powerful regulator of cardiovascular health with multiple mechanisms of action. Understanding how estrogen protects the heart and blood vessels helps explain why its decline has such profound effects on cholesterol and cardiovascular risk.
Regulation of LDL Receptor Activity
One of estrogen's most important cardiovascular functions involves the liver's LDL receptors—the proteins responsible for clearing "bad" cholesterol from the bloodstream. Research published in Arteriosclerosis, Thrombosis, and Vascular Biology demonstrated that estrogen receptors are "critically involved in the induction of hepatic LDL receptor expression" [4]. When estrogen levels are adequate, the liver produces more LDL receptors, enabling it to remove more LDL cholesterol from circulation. When estrogen declines, this clearance mechanism becomes less efficient.
Studies in human hepatoma cells have shown that 17-beta-estradiol significantly increases LDL receptor activity, enhancing the cellular uptake of LDL cholesterol [5]. This effect appears to be dose-dependent, meaning that as estrogen levels fall, so does the liver's ability to clear cholesterol from the blood.
Effects on Lipoprotein Synthesis
Beyond receptor activity, estradiol directly influences how the liver produces lipoproteins. Research has shown that 17-beta-estradiol regulates the synthesis of structural apolipoproteins for VLDL and HDL. Specifically, estrogen reduces the rate of apoB-100 synthesis (the protein that forms LDL particles) while stimulating apoA-I and apoA-II synthesis (the proteins that form protective HDL particles) [6]. This dual action helps maintain a favorable balance between harmful and protective cholesterol carriers.
PCSK9 Regulation
Recent research has revealed another mechanism by which estrogen affects cholesterol: through its influence on PCSK9, a protein that degrades LDL receptors. A study published in the Journal of Lipid Research found that circulating PCSK9 levels were 22% higher in postmenopausal women compared to premenopausal women [7]. Higher PCSK9 levels mean fewer LDL receptors available to clear cholesterol from the blood. The researchers also found that PCSK9 levels fluctuate with the menstrual cycle, correlating inversely with estrogen levels—when estrogen is higher (during ovulation), PCSK9 is lower, and LDL cholesterol tends to be reduced.
Antioxidant and Vascular Protection
Estrogen's cardiovascular benefits extend beyond cholesterol metabolism. Research has shown that estrogens inhibit the oxidation of LDL cholesterol—a critical step in the development of atherosclerosis [8]. Oxidized LDL is far more dangerous than native LDL, as it triggers inflammatory processes in arterial walls that lead to plaque formation. Additionally, estrogen promotes nitric oxide production by the vascular endothelium, which helps maintain healthy blood vessel tone and function.
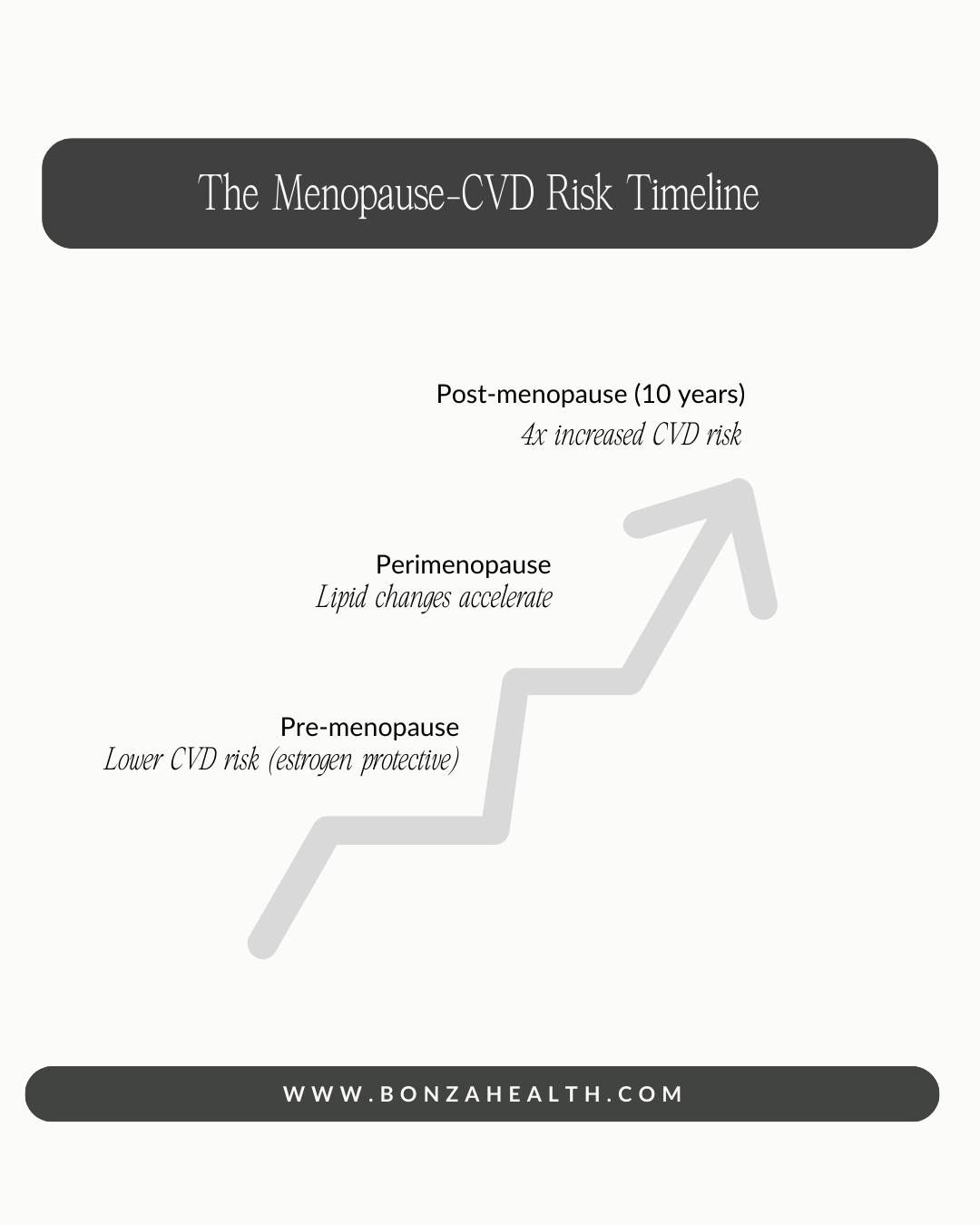
The menopause-CVD risk timeline
The Clinical Evidence: Estradiol Therapy and Lipid Improvements
The relationship between estradiol and cholesterol isn't just theoretical—clinical studies consistently demonstrate that estrogen therapy produces measurable improvements in lipid profiles. For clinicians who regularly prescribe hormone therapy, seeing cholesterol levels improve is a common and expected outcome.
A comprehensive meta-analysis published in Frontiers in Pharmacology analyzed 73 eligible studies on menopause hormone therapy and lipid profiles. The results showed that MHT significantly decreased total cholesterol (weighted mean difference: -0.43 mmol/L), LDL cholesterol (-0.47 mmol/L), and lipoprotein(a) (-49.46 mg/dL) compared to placebo or no treatment [9]. These are clinically meaningful reductions.
In a study published in Arteriosclerosis, Thrombosis, and Vascular Biology, oral hormone replacement therapy decreased total cholesterol by 14%, LDL cholesterol by 17%, and increased protective HDL cholesterol by 9% [10]. The New England Journal of Medicine published a randomized crossover trial showing that hormone therapy produced a 24% mean decrease in LDL cholesterol—a reduction comparable to some statin medications [11].
Another clinical study found that after just three months of hormone replacement therapy, fasting total cholesterol and LDL cholesterol levels were reduced by 9.8% and 16.5% respectively, while protective HDL cholesterol increased by 18.9% [12]. These improvements occur relatively quickly after initiating therapy.

Hormone therapy effects on cholesterol
Cholesterol and Cardiovascular Risk: Why This Matters
The stakes of this conversation are high. Cardiovascular disease is the leading cause of death in women, accounting for approximately 50% of female deaths [13]. Yet despite this sobering statistic, women's cardiovascular health remains systematically underappreciated and underaddressed.
Research published by the American Heart Association documents a four-fold increased risk of cardiovascular disease in women in the ten years after menopause [14]. This dramatic increase coincides precisely with the hormonal changes of the menopausal transition. Women who experience early menopause (before age 45) or premature ovarian insufficiency (before age 40) face even higher cardiovascular risks, supporting the protective role of endogenous estrogen [15].
The atherogenic lipid profile that develops after menopause—higher total cholesterol, higher LDL, higher triglycerides, and lower HDL—creates a perfect storm for cardiovascular disease development. Adding to this concern, research shows that the apolipoprotein B concentration and LDL-C/apoB ratio increase significantly in postmenopausal women, often converging with and exceeding the values seen in men by age 50-55 [16].

Blood pressure, blood sugar, family history, and lifestyle factors can all impact CVD risk. A comprehensive assessment helps determine the best treatment approach.
The Problem: Women's Cardiovascular Health Is Underdiagnosed
Here's where the frustration for many women intensifies. Despite the clear scientific evidence linking menopause, estrogen decline, and cardiovascular risk, women's heart disease remains what researchers call "understudied, under-recognized, underdiagnosed, and undertreated" [17].
A 2024 review noted that cardiovascular disease in women "remains underdiagnosed, undertreated, and portends worse outcomes in women than men" [18]. Women are less likely to receive diagnostic imaging, less likely to receive appropriate interventions, and more likely to have their symptoms dismissed or attributed to non-cardiac causes [19].
The dismissive "it's just aging" response to rising cholesterol in menopausal women exemplifies this broader pattern. While age is certainly a cardiovascular risk factor, attributing lipid changes solely to aging ignores the biological reality that hormonal status—specifically estrogen levels—is a major driver of these metabolic shifts. This distinction matters because it points toward a potential intervention beyond (or in addition to) statin therapy.
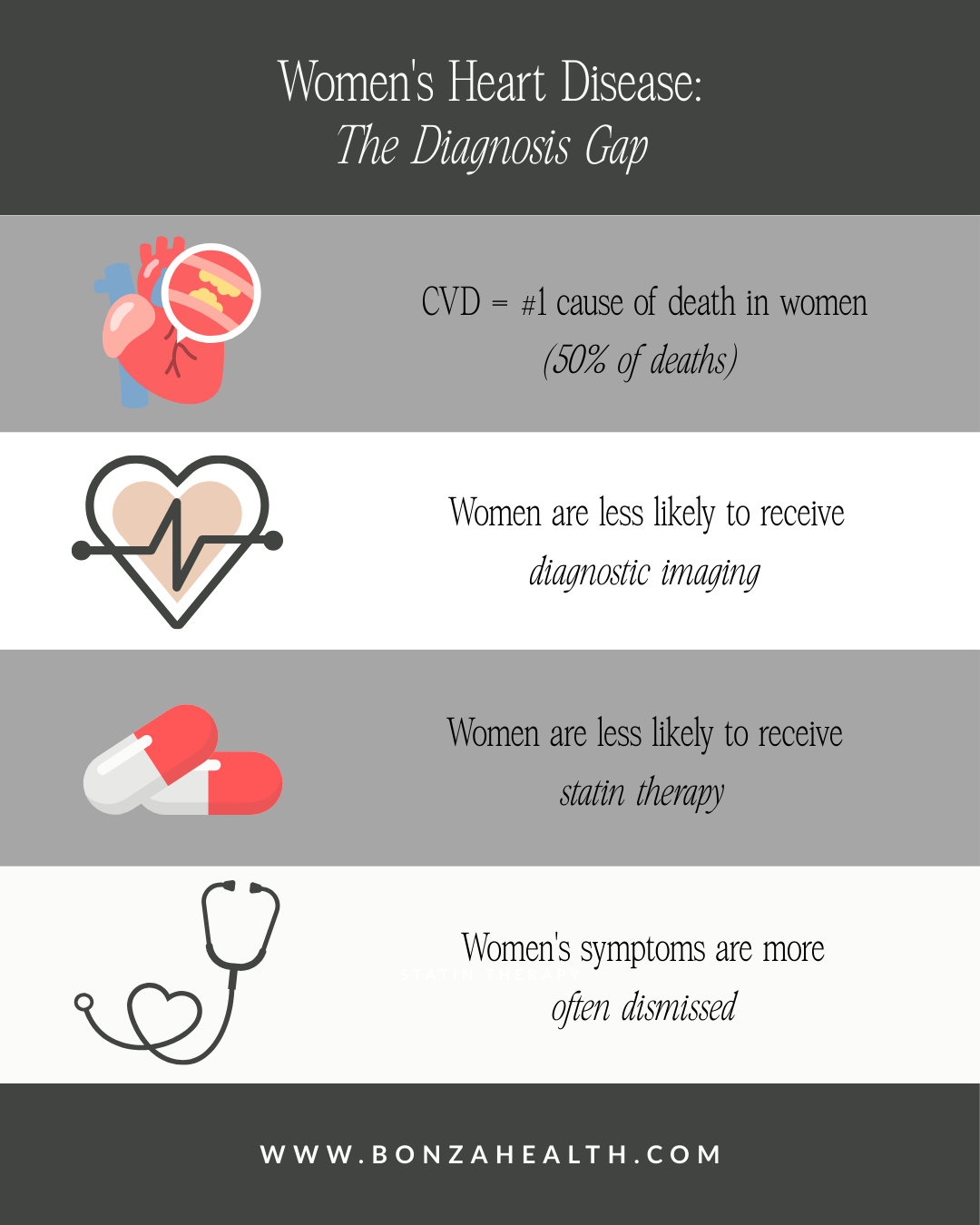
Women’s heart disease: the diagnosis gap
A More Complete Picture: Individualized Care
This is not to suggest that every woman should take estrogen or that hormone therapy is appropriate for everyone. The decision to use hormone therapy is individual and depends on many factors, including a woman's symptoms, risk factors, personal and family history, and preferences. However, what the research clearly supports is that estrogen's role in cholesterol metabolism deserves consideration in the clinical conversation.
Current evidence supports that menopausal hormone therapy may reduce cardiovascular morbidity and mortality when commenced during the early postmenopausal period—within ten years of the final menstrual period or before age 60 [16]. The "timing hypothesis" suggests that the cardiovascular effects of hormone therapy depend heavily on when it is initiated relative to menopause.
It's also worth noting that different formulations and routes of administration have different effects. Transdermal estradiol, for example, does not increase triglycerides the way oral estrogen can, and may even reduce them [20]. Research shows transdermal estradiol leads to favorable changes in major cardiovascular risk factors while avoiding some of the concerns associated with oral formulations [21].

When estrogen declines at menopause, cholesterol metabolism changes—often dramatically.
Advocating for Your Cardiovascular Health
If your cholesterol numbers have risen with menopause, you deserve more than a shrug and a prescription pad. You deserve a thoughtful conversation about the hormonal changes driving those numbers and the range of options available to address them. Here are some points to discuss with your healthcare provider:
Consider the timing. When did your cholesterol begin to change relative to your menopausal transition? A clear temporal relationship supports the hormonal connection.
Evaluate your complete risk profile. Cholesterol is just one piece of cardiovascular risk. Blood pressure, blood sugar, family history, and lifestyle factors all matter. A comprehensive assessment helps determine the best approach.
Discuss all your options. Statins are one tool, but they're not the only one. Lifestyle modifications, hormone therapy (if appropriate), and other interventions may all have roles to play.
Ask about the whole picture. If you're experiencing menopausal symptoms like hot flashes or sleep disturbances, and you're also seeing cholesterol changes, these may be connected manifestations of the same underlying hormonal shift.
The science is clear: estrogen plays a vital role in maintaining healthy cholesterol levels and protecting against cardiovascular disease. When estrogen declines at menopause, cholesterol metabolism changes—often dramatically. This isn't a mystery, and it isn't "just aging." It's biology, and it deserves to be recognized as such in your medical care.

References
[1] S. R. Kilim and S. R. Chandala, "A comparative study of lipid profile and oestradiol in pre- and post-menopausal women," J. Clin. Diagn. Res., vol. 7, no. 8, pp. 1596–1598, 2013. https://doi.org/10.7860/JCDR/2013/6162.3234
[2] K. A. Matthews et al., "Changes in cardiovascular risk factors during the perimenopause and postmenopause and carotid artery atherosclerosis in healthy women," Stroke, vol. 32, no. 5, pp. 1104–1111, 2001. https://doi.org/10.1161/01.STR.32.5.1104
[3] I. C. D. Westendorp et al., "Menopausal status and risk factors for cardiovascular disease," Maturitas, vol. 33, no. 2, pp. 117–123, 1999. https://doi.org/10.1016/S0378-5122(99)00046-0
[4] P. Parini, B. Angelin, and M. Rudling, "Importance of estrogen receptors in hepatic LDL receptor regulation," Arterioscler. Thromb. Vasc. Biol., vol. 17, no. 9, pp. 1800–1805, 1997. https://doi.org/10.1161/01.ATV.17.9.1800
[5] A. J. Owen and M. Abbey, "Regulation of low-density lipoprotein receptor activity by estrogens and phytoestrogens in a HepG2 cell model," Ann. Nutr. Metab., vol. 48, no. 4, pp. 269–275, 2004. https://doi.org/10.1159/000080463
[6] B. T. Palmisano, L. Zhu, and J. M. Stafford, "Role of estrogens in the regulation of liver lipid metabolism," Adv. Exp. Med. Biol., vol. 1043, pp. 227–256, 2017. https://doi.org/10.1007/978-3-319-70178-3_12
[7] M. Ghosh, C. Gälman, M. Rudling, and B. Angelin, "Influence of physiological changes in endogenous estrogen on circulating PCSK9 and LDL cholesterol," J. Lipid Res., vol. 56, no. 2, pp. 463–469, 2015. https://doi.org/10.1194/jlr.M055780
[8] N. K. Wenger, "Cardiovascular effects of estrogen and lipid-lowering therapies in postmenopausal women," Circulation, vol. 93, no. 10, pp. 1928–1937, 1996. https://doi.org/10.1161/01.CIR.93.10.1928
[9] X. Chen et al., "The effects of menopause hormone therapy on lipid profile in postmenopausal women: A systematic review and meta-analysis," Front. Pharmacol., vol. 13, p. 850815, 2022. https://doi.org/10.3389/fphar.2022.850815
[10] T. S. Mikkola et al., "Hormone replacement therapy lowers plasma Lp(a) concentrations," Arterioscler. Thromb. Vasc. Biol., vol. 16, no. 10, pp. 1215–1221, 1996. https://doi.org/10.1161/01.ATV.16.10.1215
[11] G. M. Darling et al., "Estrogen and progestin compared with simvastatin for hypercholesterolemia in postmenopausal women," N. Engl. J. Med., vol. 337, no. 9, pp. 595–601, 1997. https://doi.org/10.1056/NEJM199708283370903
[12] M. Weintraub et al., "Hormone replacement therapy enhances postprandial lipid metabolism in postmenopausal women," Metabolism, vol. 48, no. 9, pp. 1193–1198, 1999. https://doi.org/10.1016/S0026-0495(99)90137-0
[13] P. Anagnostis et al., "Menopause-associated risk of cardiovascular disease," Endocr. Connect., vol. 11, no. 4, p. e210537, 2022. https://doi.org/10.1530/EC-21-0537
[14] C. Schenck-Gustafsson, "Menopause, cholesterol and cardiovascular disease," Menopause Int., vol. 13, no. 1, pp. 19–22, 2007. https://doi.org/10.1258/175404507780456755
[15] A. Kaczmarek et al., "Menopause and women's cardiovascular health: is it really an obvious relationship?," Menopause Rev., vol. 22, no. 1, pp. 1–8, 2023. https://doi.org/10.5114/pm.2023.125234
[16] S. R. El Khoudary et al., "Menopause transition and cardiovascular disease risk: Implications for timing of early prevention: A scientific statement from the American Heart Association," Circulation, vol. 142, no. 25, pp. e506–e532, 2020. https://doi.org/10.1161/CIR.0000000000000912
[17] N. K. Wenger et al., "Call to action for cardiovascular disease in women: epidemiology, awareness, access, and delivery of equitable health care," Circulation, vol. 145, no. 23, pp. e1059–e1071, 2022. https://doi.org/10.1161/CIR.0000000000001071
[18] L. S. Mehta et al., "Cardiovascular disease risk factors in women: the impact of race and ethnicity," Circulation, vol. 147, no. 19, pp. 1471–1487, 2023. https://doi.org/10.1161/CIR.0000000000001139
[19] D. Appiah and P. J. Schreiner, "Cardiovascular disease in older women," Clin. Geriatr. Med., vol. 37, no. 4, pp. 565–584, 2021. https://doi.org/10.1016/j.cger.2021.05.005
[20] T. Vaisar et al., "Perimenopausal transdermal estradiol replacement and cardiovascular risk factors," J. Clin. Lipidol., vol. 15, no. 1, pp. 151–161, 2021. https://doi.org/10.1016/j.jacl.2020.11.009
[21] I. F. Godsland, "Effects of postmenopausal hormone replacement therapy on lipid, lipoprotein, and apolipoprotein (a) concentrations," Steroids, vol. 66, no. 3-5, pp. 429–447, 2001. https://doi.org/10.1016/S0039-128X(00)00167-0