
The Great Mimicker: When Hashimoto's Hides in Perimenopause
Written and edited by Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Hashimoto's thyroiditis is the "Great Mimicker" of perimenopause.
Michelle, 46, came to my office exhausted. She hadn't slept through the night in months. She was losing clumps of hair in the shower. She'd gained fifteen pounds despite no changes in diet or exercise. Her brain fog was so bad she'd forgotten her son's basketball game—something she'd never done before.
"I know what this is," she told me. "I'm perimenopausal. My mom went through early menopause with the same symptoms. I just need you to confirm it."
Her previous doctor had checked her TSH six months earlier. "Normal," she'd been told. "Within range." But when I ran a comprehensive thyroid panel, her TPO antibodies came back at 287 IU/mL—a clear sign of Hashimoto's thyroiditis, an autoimmune condition attacking her thyroid that had been silently progressing while everyone blamed her symptoms on aging.
Michelle's story is not unique. I see women like her almost weekly. And it's why I call Hashimoto's thyroiditis the "Great Mimicker" of perimenopause.
When "Normal" Isn't Normal at All
For many women in their 40s, the "midlife shift" begins with a specific brand of exhaustion: the kind that coffee can't fix and a full night's sleep barely touches. Usually, the first suspect is perimenopause. And while declining estrogen is often to blame, there is a "Great Mimicker" lurking in the background for millions of women: Hashimoto's Thyroiditis.
In my practice at Bonza Health, I frequently see women who have been told by other providers that their labs are "normal" and their symptoms are just an inevitable part of aging. However, when we dig deeper, we find that the ovaries aren't the only glands struggling; the thyroid is under attack.

Fatigue, brain fog, hair loss, and weight changes are common symptoms of both Hashimoto’s and perimenopause.
The Perfect Storm of Overlapping Symptoms
Perimenopause and hypothyroidism share a Venn diagram that is almost a circle. Both conditions can cause weight gain, brain fog, mood changes, thinning hair, and dry skin. A 2024 study in Scientific Reports demonstrated that Hashimoto's patients—even with normal hormone levels—experience significantly more fatigue, forgetfulness, anxiety, depression, dry skin, and hair loss than healthy controls [1]. These symptoms correlated directly with elevated TPO antibody levels and inflammatory markers.
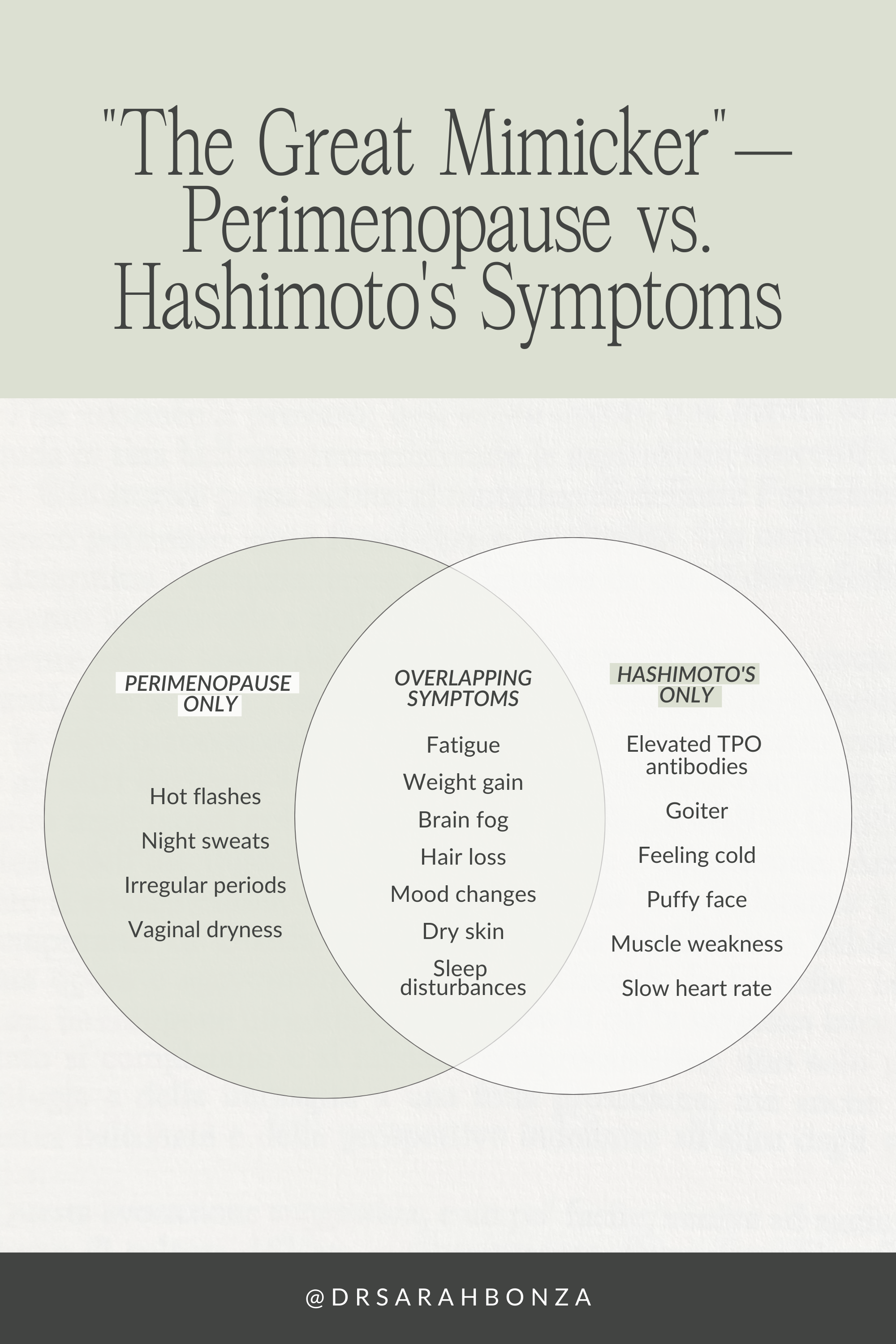
Both Hashimoto’s and perimenopausecan cause weight gain, brain fog, mood changes, thinning hair, and dry skin.
Why TSH Alone is Often a False Reassurance
The standard of care in many clinics is to test only TSH. However, Hashimoto's is an autoimmune condition. In early stages, the thyroid may still produce enough hormone to keep TSH "normal," but the body is already inflamed due to TPO antibodies. Research confirms that patients with TPO antibodies experience significant symptoms long before their TSH becomes abnormal [2].
A systematic review found compelling evidence that thyroid autoimmunity itself—independent of hormone status—may be responsible for ongoing symptoms [3]. This is why testing only TSH fails so many perimenopausal women.

The standard of care in many clinics is to test only TSH. However, a comprehensive review includes a full thyroid panel (TSH, Free T3, Free T4, Reverse T3, TPO/Tg antibodies), metabolic markers, hormone assessment, and nutrient status (vitamin D, selenium, zinc, iron, ferritin).
The Estrogen-Thyroid Connection
Estrogen increases Thyroid-Binding Globulin (TBG), the protein that carries thyroid hormone through your blood. When estrogen fluctuates wildly during perimenopause, more thyroid hormone may be bound up and unavailable for your cells—creating "functional hypothyroidism" where you have symptoms despite normal-looking labs [4]. Additionally, hormonal fluctuations can trigger or exacerbate autoimmune responses, making perimenopausal women particularly vulnerable to developing or worsening Hashimoto's [5].
How Hashimoto's Impacts Your Hair
Hair loss is one of the most distressing symptoms for women with thyroid dysfunction. Thyroid hormones are essential for hair follicle growth and maintenance, extending the anagen (growth) phase and stimulating hair matrix proliferation [6]. When hypothyroidism develops, patients experience diffuse hair loss, dry and brittle hair, and the classic loss of the lateral third of the eyebrows.
A 2023 review highlighted that hypothyroidism impedes epidermal cell division, leading to premature entry into the catagen phase and delayed hair regrowth [7]. Importantly, alopecia areata shares a common autoimmune background with Hashimoto's; a meta-analysis found Hashimoto's has an odds ratio of 4.31 for association with alopecia areata [8]. This underscores why comprehensive thyroid testing is essential for any woman presenting with hair loss during perimenopause.

Hair loss is one of the most distressing symptoms for women with thyroid dysfunction.
Nutritional Support for Thyroid Health
Selenium
Selenium is essential for thyroid hormone synthesis and exerts powerful antioxidant effects. A 2024 meta-analysis of 35 randomized controlled trials (2,358 participants) found that selenium supplementation significantly decreases TPO antibody levels and reduces TSH in patients not on thyroid hormone replacement [9]. Selenomethionine appears more effective than other forms, with improvements seen at 3-6 months [10].
Zinc
Zinc regulates deiodinase enzyme activity (converting T4 to active T3) and TSH synthesis [11]. Zinc deficiency can contribute to hypothyroidism, while hypothyroidism reduces zinc absorption: a vicious cycle. A striking case report demonstrated that hair loss from hypothyroidism may not improve with thyroxine alone unless zinc is added [12]. A randomized trial confirmed that zinc and selenium co-supplementation improves thyroid function in hypothyroid women [13].
Vitamin D
Vitamin D deficiency is linked to higher thyroid autoimmunity prevalence. A 2021 meta-analysis found that vitamin D supplementation significantly reduced both TPO-Ab and TG-Ab titers, with effects seen after 3+ months of supplementation [14]. Vitamin D's immunomodulatory properties help control autoimmunity by reducing pro-inflammatory cytokines [15]. Given its low cost and minimal side effects, optimizing vitamin D should be foundational for Hashimoto's patients.
Iron and Other Considerations
Normal iron levels may improve thyroid function and reduce antibodies [16]. Iron is required for thyroid peroxidase enzyme activity, and iron deficiency—common in perimenopausal women—compounds thyroid dysfunction. A note of caution: excess iodine tends to worsen Hashimoto's in iodine-replete areas, so iodine should not be supplemented without documented deficiency [16].
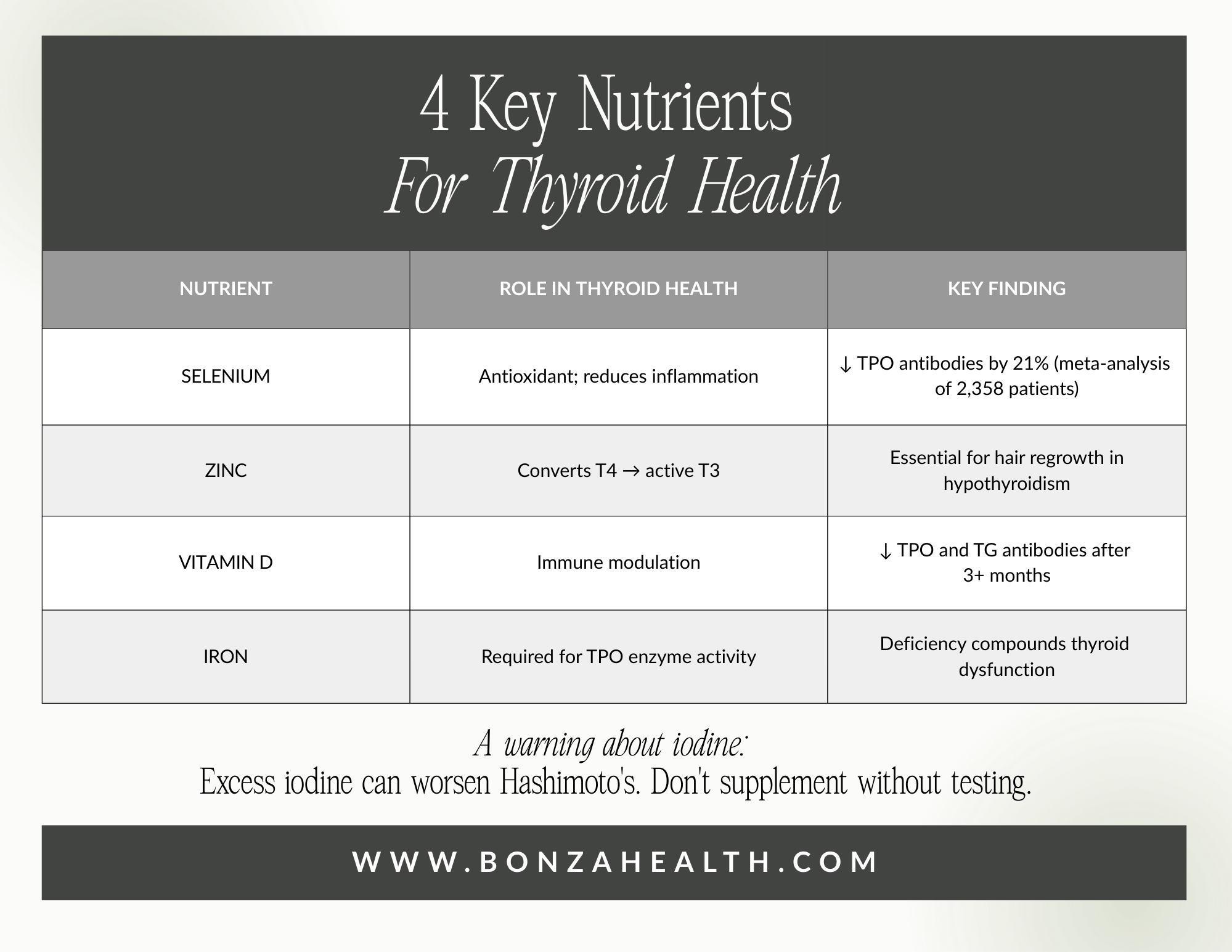
Selenium, zinc, vitamin D, and iron are all necessary for thyroid health.
When to Consider Thyroid Hormone Replacement
Current guidelines from the American Thyroid Association and AACE recommend treatment when TSH is consistently above 10 mIU/L, or between 4.5-10 mIU/L with positive TPO antibodies and symptoms [17]. For women pregnant or trying to conceive, treatment is recommended if TSH exceeds trimester-specific ranges. Cardiovascular risk factors also influence treatment decisions.
For subclinical hypothyroidism (TSH <10 mIU/L), a "wait and watch" approach is often appropriate, with repeat testing in 2-3 months [18]. However, symptoms affecting quality of life, positive TPO antibodies, or cardiovascular risk may tip the balance toward treatment, especially in younger patients [19].

When to start thyroid hormone replacement therapy varies depending on the specific situation.
Functional Medicine vs. Traditional Medicine Approaches
Traditional medicine typically monitors TSH and treats with levothyroxine when overt hypothyroidism develops, with little attention to antibody levels or the underlying autoimmune process. Functional medicine takes a more comprehensive approach:
Complete Thyroid Panel: Free T3, Free T4, Reverse T3, and TPO/TG antibodies: not just TSH.
Optimal vs. Normal Ranges: Aiming for TSH of 1.0-2.5 mIU/L rather than accepting 4.5-5.0 as "normal."
Nutrient Optimization: Testing and optimizing selenium, zinc, vitamin D, and iron.
Gut Health: Addressing intestinal health, as Hashimoto's is associated with gastric disorders in 10-40% of patients [16].
Combination Therapy Consideration: For patients symptomatic despite normalized TSH, some consider T4/T3 combination therapy. About 20% of athyreotic patients don't maintain normal Free T3 on T4 monotherapy [20]. The ATA notes insufficient evidence for routine combination therapy, but the European Thyroid Association suggests it may be considered experimentally in select patients.

Functional medicine takes a comprehensive approach to treating hypothyroidism and Hashimoto’s.
The Bonza Health Investigative Approach
At Bonza Health, we don't guess; we test. A comprehensive review includes a full thyroid panel (TSH, Free T3, Free T4, Reverse T3, TPO/Tg antibodies), metabolic markers, hormone assessment, and nutrient status (vitamin D, selenium, zinc, iron, ferritin). By identifying Hashimoto's early—even before overt hypothyroidism develops—we can implement interventions that may slow disease progression and improve quality of life.
Six months after her diagnosis, Michelle's story had changed. With optimized vitamin D, selenium, zinc, and a low dose of levothyroxine, she was sleeping again. Her hair was growing back. She'd lost eight pounds. "I thought this was just what being in my mid-forties felt like," she told me. "I'm so grateful we looked deeper."
Conclusion
Hashimoto's thyroiditis truly is the "Great Mimicker" of perimenopause. Its symptoms—fatigue, weight gain, brain fog, mood changes, hair loss, dry skin—are easily attributed to declining estrogen. But for millions of women, an autoimmune attack on the thyroid is silently progressing, driving inflammation and symptoms that a simple TSH test may miss entirely.
If you're a perimenopausal woman told your symptoms are "just aging", or your labs are "normal," consider requesting comprehensive thyroid testing including TPO antibodies. Optimizing selenium, zinc, vitamin D, and iron may provide meaningful relief. And if thyroid hormone replacement becomes necessary, work with a provider who understands personalized treatment.
Your fatigue, hair loss, and brain fog deserve more than dismissal. They deserve investigation, understanding, and effective treatment.

Discover the Bonza Health Method, our 3-step system helping women navigate perimenopause.
References
[1] L. Song et al., "Thyroid antibodies in Hashimoto's thyroiditis patients are positively associated with inflammation and multiple symptoms," Sci. Rep., vol. 14, 2024, doi: 10.1038/s41598-024-78938-7.
[2] T. G. Strieder et al., "Prediction of progression to overt hypothyroidism," J. Clin. Endocrinol. Metab., vol. 88, no. 6, pp. 2667-2672, 2003.
[3] E. M. Koning et al., "Persisting symptoms in patients with Hashimoto's disease despite normal thyroid hormone levels," J. Transl. Autoimmun., vol. 4, 2021, doi: 10.1016/j.jtauto.2021.100101.
[4] A. P. Santin and T. W. Furlanetto, "Role of estrogen in thyroid function and growth," J. Thyroid Res., vol. 2011, 2011, doi: 10.4061/2011/875125.
[5] I. Muller et al., "The interplay between thyroid function and the female reproductive system," Nat. Rev. Endocrinol., vol. 17, pp. 476-489, 2021.
[6] L. Poppe et al., "Study of the Thyroid Profile of Patients with Alopecia," J. Clin. Med., vol. 12, no. 3, p. 1115, 2023, doi: 10.3390/jcm12031115.
[7] A. Bani Ali et al., "Impact of Thyroid Dysfunction on Hair Disorders," Cureus, vol. 15, no. 8, p. e43266, 2023, doi: 10.7759/cureus.43266.
[8] J. W. Shin et al., "A systematic review and meta-analysis of alopecia areata-related comorbidities," J. Am. Acad. Dermatol., 2023.
[9] V. V. Huwiler et al., "Selenium Supplementation in Patients with Hashimoto Thyroiditis: A Systematic Review and Meta-Analysis," Thyroid, vol. 34, no. 3, pp. 295-313, 2024, doi: 10.1089/thy.2023.0556.
[10] H. Zhang et al., "Clinical efficacy of selenium supplementation in patients with Hashimoto thyroiditis," Medicine, vol. 104, no. 35, p. e44043, 2025.
[11] J. S. Severo et al., "The Role of Zinc in Thyroid Hormones Metabolism," Int. J. Vitam. Nutr. Res., vol. 89, no. 1-2, pp. 80-88, 2019, doi: 10.1024/0300-9831/a000262.
[12] A. Betsy et al., "Zinc Deficiency Associated with Hypothyroidism: An Overlooked Cause of Severe Alopecia," Int. J. Trichology, vol. 5, no. 1, pp. 40-42, 2013, doi: 10.4103/0974-7753.114714.
[13] S. Mahmoodianfard et al., "Effects of Zinc and Selenium Supplementation on Thyroid Function in Hypothyroid Female Patients," J. Am. Coll. Nutr., vol. 34, no. 5, pp. 391-399, 2015.
[14] J. Zhang et al., "Effects of vitamin D on thyroid autoimmunity markers in Hashimoto's thyroiditis," J. Int. Med. Res., vol. 49, no. 12, 2021, doi: 10.1177/03000605211060675.
[15] J. Filipowska et al., "Impact of Vitamin D on Immunopathology of Hashimoto's Thyroiditis," Nutrients, vol. 15, no. 14, p. 3174, 2023, doi: 10.3390/nu15143174.
[16] K. A. Zeller and E. K. Lee, "Hashimoto Thyroiditis," in StatPearls, Treasure Island, FL: StatPearls Publishing, 2024.
[17] D. S. Cooper, "Clinical practice. Subclinical hypothyroidism," N. Engl. J. Med., vol. 345, no. 4, pp. 260-265, 2001.
[18] J. R. Garber et al., "Clinical Practice Guidelines for Hypothyroidism in Adults," Endocr. Pract., vol. 18, no. 6, pp. 988-1028, 2012.
[19] C. Stott et al., "To Treat or Not to Treat Subclinical Hypothyroidism," J. Clin. Med., vol. 9, no. 2, p. 299, 2020, doi: 10.3390/jcm9020299.
[20] D. S. Ross, "Treating hypothyroidism is not always easy," J. Intern. Med., vol. 291, no. 2, pp. 128-143, 2022, doi: 10.1111/joim.13410.