
Menopausal Hormone Therapy and Cancer in Women: Evidence-Based Guidance
Written and edited by Sarah Bonza MD, MPH, MSCP, FAAFP, DipABLM, NBC-HWC

Menopausal hormone therapy (MHT) remains one of the most debated topics in women’s health, especially for those with a personal or family history of cancer. This blog reviews the evidence, highlights the work of Dr. Avrum Bluming, and provides a clear, practical chart for clinicians and patients navigating MHT in the context of cancer risk.
Dr. Avrum Bluming’s Contributions to Menopause Hormone Therapy
Dr. Avrum Bluming, a leading breast oncologist and author of Estrogen Matters, has been instrumental in challenging misconceptions about MHT and cancer, especially breast cancer. His research and advocacy underscore several key points:
Estrogen alone does not increase breast cancer risk and may even reduce it
Dr. Bluming cites large studies and meta-analyses showing that estrogen-only therapy is not associated with an increased risk of breast cancer, and may decrease both breast cancer incidence and mortality.[1,2]
Progesterone, not estrogen, is the primary concern for breast cancer risk
The addition of synthetic progestins, rather than natural micronized progesterone, is associated with an increased risk of breast cancer.[3,4]
Menopause hormone therapy is safe for some breast cancer survivors
Menopause hormone therapy can be considered in select breast cancer survivors, especially those with hormone receptor (HR)-negative tumors. MHT is a good option when quality of life is significantly diminished and non-hormonal options have failed.[1,5,6]
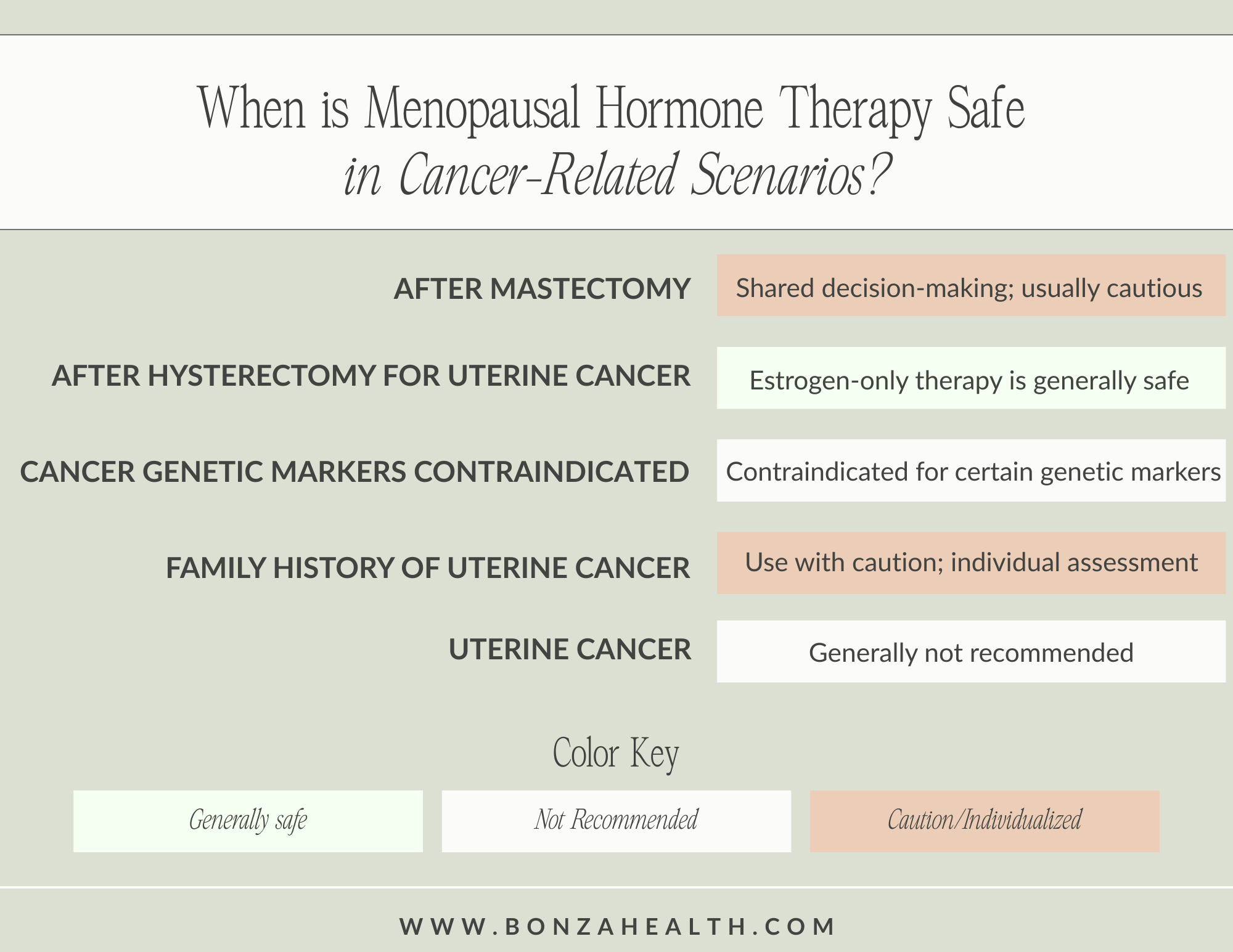
When is Menopausal Hormone Therapy Safe?
The following chart summarizes current evidence and expert recommendations on the use of MHT in various cancer-related scenarios. These recommendations include those of Dr. Bluming, the North American Menopause Society (NAMS), and the American Cancer Society:
Evidence-Based Prescribing Recommendations for Menopause Hormone Therapy
When it comes to MHT and cancer risk, the formulation of the therapy used matters. Some formulations are associated with an increased risk of breast cancer, while others appear to reduce the risk.
Studies show that progesterone (especially synthetic progestins) is the main driver of increased breast cancer risk in combined MHT, not estrogen.[3,4] Micronized (bioidentical) progesterone is associated with a much lower risk than synthetic progestins, and may even be protective against breast cancer.[3,4]
Estrogen-only therapy (for women without a uterus) is not associated with increased breast cancer risk. MHT may even lower the risk of breast cancer.[2,4]
Let’s take a closer look at what research says about menopause hormone therapy and cancer risk.

MHT & Breast Cancer
Estrogen Alone
When used alone, estrogen does not increase the risk of breast cancer. Studies show it may even decrease the risk of breast cancer.[1] Estrogen-alone therapy may also be considered in women with severe menopausal symptoms and no uterus.
Estrogen + Progestin
Estrogen plus progestin (a synthetic form of progesterone) therapy is associated with a higher risk of breast cancer, especially with long-term use.[3,7]
Estrogen + Micronized Progesterone
Breast cancer risk with the use of estrogen plus micronized progesterone is much lower than with synthetic progestins. Some studies show no increased risk of breast cancer with estrogen plus micronized progesterone, and possibly a reduced risk.[3,4]
Other Considerations for Breast Cancer:
For some women with a personal or family history of breast cancer, MHT may be contraindicated. Possible contraindications for MHT include:
Breast Cancer Survivors: MHT is generally not recommended, especially for HR-positive tumors. However, MHT may be considered in HR-negative cases after shared decision-making, and when non-hormonal therapies have failed.[6,8]
Family History of Breast Cancer/BRCA Mutation: MHT does not appear to increase the relative risk of breast cancer. However, family history should be considered in counseling.[8]

MHT & Uterine Cancer
History of Uterine Cancer
Systemic MHT is generally not recommended for women with a history of uterine cancer, especially hormone-sensitive cancers.[9] After hysterectomy for uterine cancer, estrogen-only therapy is generally safe.[7,9]
Family History of Uterine Cancer
An individualized assessment is necessary for women with a family history of uterine cancer. Some risk may exist, but it’s not an absolute contraindication.
Genetic Markers (BRCA1/2, Lynch)
Due to the high risk of hormone-driven cancers, MHT is contraindicated for women with certain genetic variants such as BRCA1, BRCA2, and Lynch syndrome.
MHT & Other Cancers
Ovarian Cancer
There is a small increased risk of ovarian cancer with both estrogen and combined therapy. The absolute risk is low and dissipates after stopping MHT.[8] However, MHT is not recommended in hormone-dependent ovarian cancers.
Colorectal Cancer
Studies show that MHT may reduce the risk of colon cancer.[7,8]
Cervical Cancer
MHT can be used safely among women with cervical cancer, as cervical cancer is not hormone-sensitive.[9]

Clinical Takeaways
Personalized, shared decision-making is essential. Consider the type of cancer, hormone receptor status, patient preferences, and symptom severity.
Estrogen alone is generally safe for women without a uterus, including after hysterectomy for uterine cancer.
Progesterone choice matters: Prefer micronized progesterone over synthetic progestins to minimize breast cancer risk.
Women with genetic cancer syndromes (BRCA1/2, Lynch) should avoid MHT.
For breast cancer survivors, MHT is generally not recommended but may be considered in HR-negative cases with severe symptoms, after full discussion with oncology.

References
[1] Alloy. Menopause, breast cancer, and what comes next-a conversation with Dr. Avrum Bluming. https://www.myalloy.com/blog/menopause-breast-cancer-and-what-comes-next
[2] Balance. Getting to the truth around HRT and breast cancer with Dr Avrum Bluming. https://www.balance-menopause.com/menopause-library/getting-to-the-truth-around-hrt-and-breast-cancer-with-dr-avrum-bluming/
[3] Abenhaim HA, Suissa S, Azoulay L, Spence AR, Czuzoj-Shulman N, Tulandi T. Menopausal Hormone Therapy Formulation and Breast Cancer Risk. Obstet Gynecol. 2022;139(6):1103-1110. https://doi.org/10.1097/aog.0000000000004723
[4] Saul H, Gursul D, Cassidy S, Vinogradova Y. Risk of breast cancer with HRT depends on therapy type and duration. BMJ. 2022;376:o485. Published 2022 Mar 8. https://doi.org/10.1136/bmj.o485
[5] Bluming AZ. Hormone Replacement Therapy After Breast Cancer: It Is Time. Cancer J. 2022;28(3):183-190. https://doi.org/10.1097/ppo.0000000000000595
[6] Coronado PJ, Gómez A, Iglesias E, et al. Eligibility criteria for using menopausal hormone therapy in breast cancer survivors: a safety report based on a systematic review and meta-analysis. Menopause. 2024;31(3):234-242. https://doi.org/10.1097/gme.0000000000002317
[7] American Cancer Society. Menopausal hormone therapy and cancer risk. https://www.cancer.org/cancer/risk-prevention/medical-treatments/menopausal-hormone-replacement-therapy-and-cancer-risk.html
[8] ObG Project. North American Menopause Society: hormone therapy statement. https://www.obgproject.com/2022/11/21/north-american-menopause-society-releases-2017-hormone-therapy-statement/
[9] Kotait M, Shea A, Nguyen JMV. Menopausal hormone therapy in patients with a history of gynecologic cancer. CMAJ. 2023;195(49):E1721. Published 2023 Dec 17. https://doi.org/10.1503/cmaj.231066