
DEXA Scans in Perimenopausal Women: The Case for Earlier Bone Health Screening
Written and edited by Sarah Bonza MD, MPH, MSCP, FAAFP, DipABLM, NBC-HWC

As women navigate the transformative journey of perimenopause, many focus on managing hot flashes, mood changes, and sleep disturbances while overlooking one of the most significant health risks occurring beneath the surface: accelerated bone loss.[1]
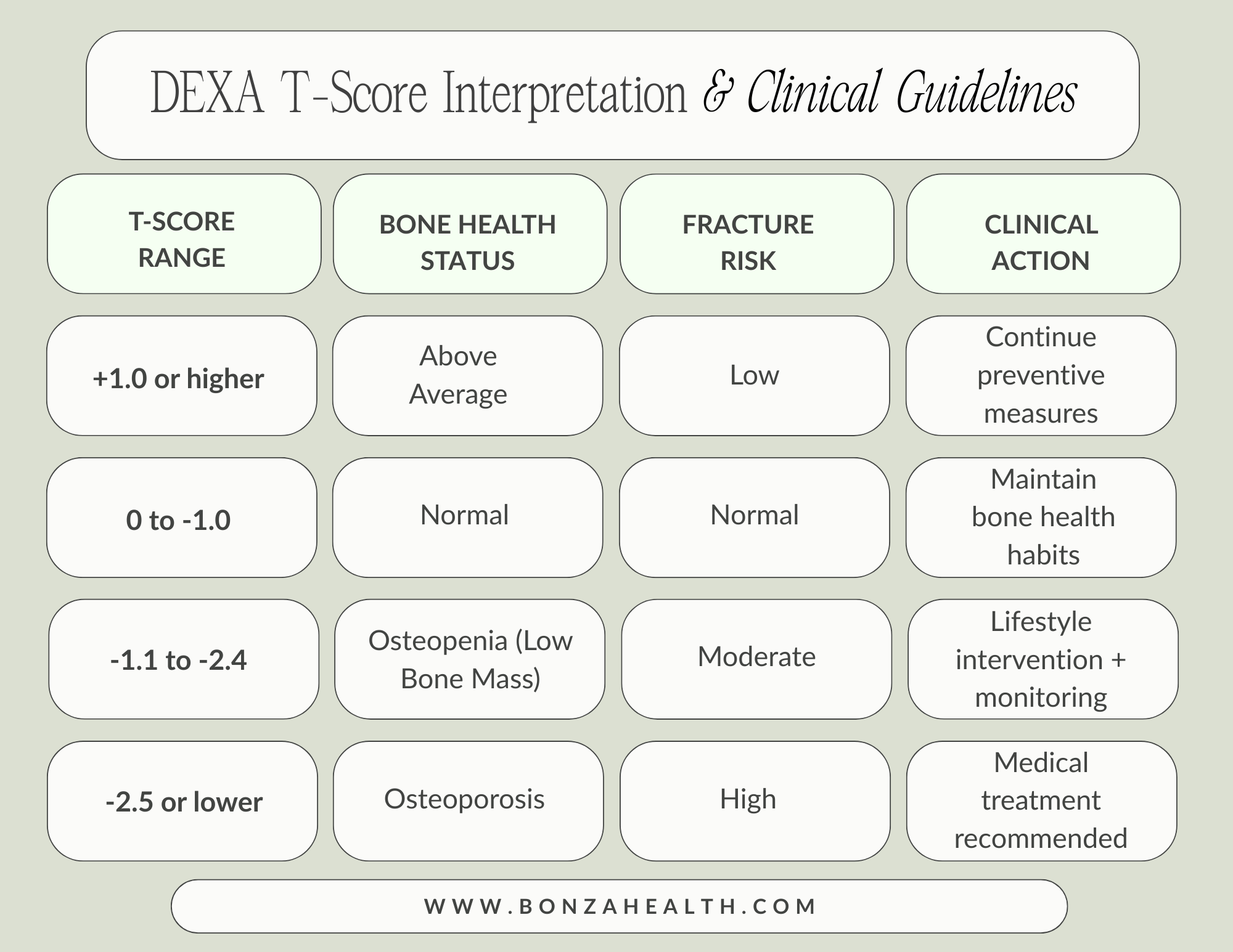
The current medical paradigm typically recommends bone density screening through dual-energy X-ray absorptiometry (DEXA) scans beginning at age 65, yet mounting evidence suggests that the most critical period for bone health occurs much earlier: during the perimenopausal transition.[1-3]
Understanding the Perimenopause-Bone Health Connection
The Hidden Crisis of Bone Loss
The perimenopausal transition represents a critical window for bone health that has been largely underappreciated in clinical practice.[2] Research from the Study of Women's Health Across the Nation (SWAN), the largest prospective study examining bone changes during menopause, reveals startling findings about the timing and magnitude of bone loss.[1,2]
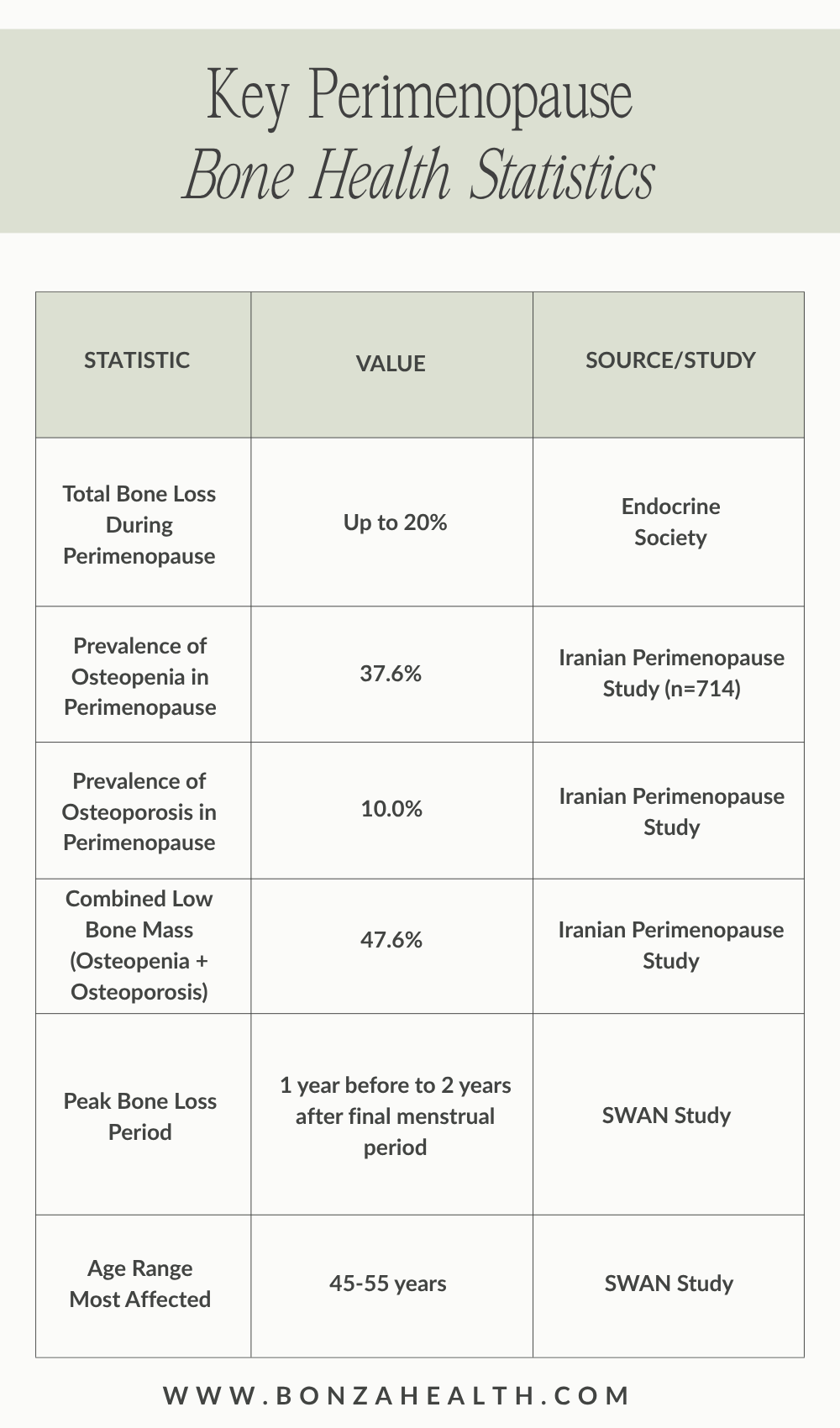
Women can lose up to 20% of their bone density during their perimenopausal years, with the most dramatic losses occurring in a narrow 3-year window around the final menstrual period.[1,2,4]
The SWAN study documented that bone loss begins approximately 1-2 years before the final menstrual period and continues at accelerated rates for the first two years after menopause, with annual spine bone density losses of 2.5% and femoral neck losses of 1.8% in white women.[2,3]
The Estrogen-Bone Connection
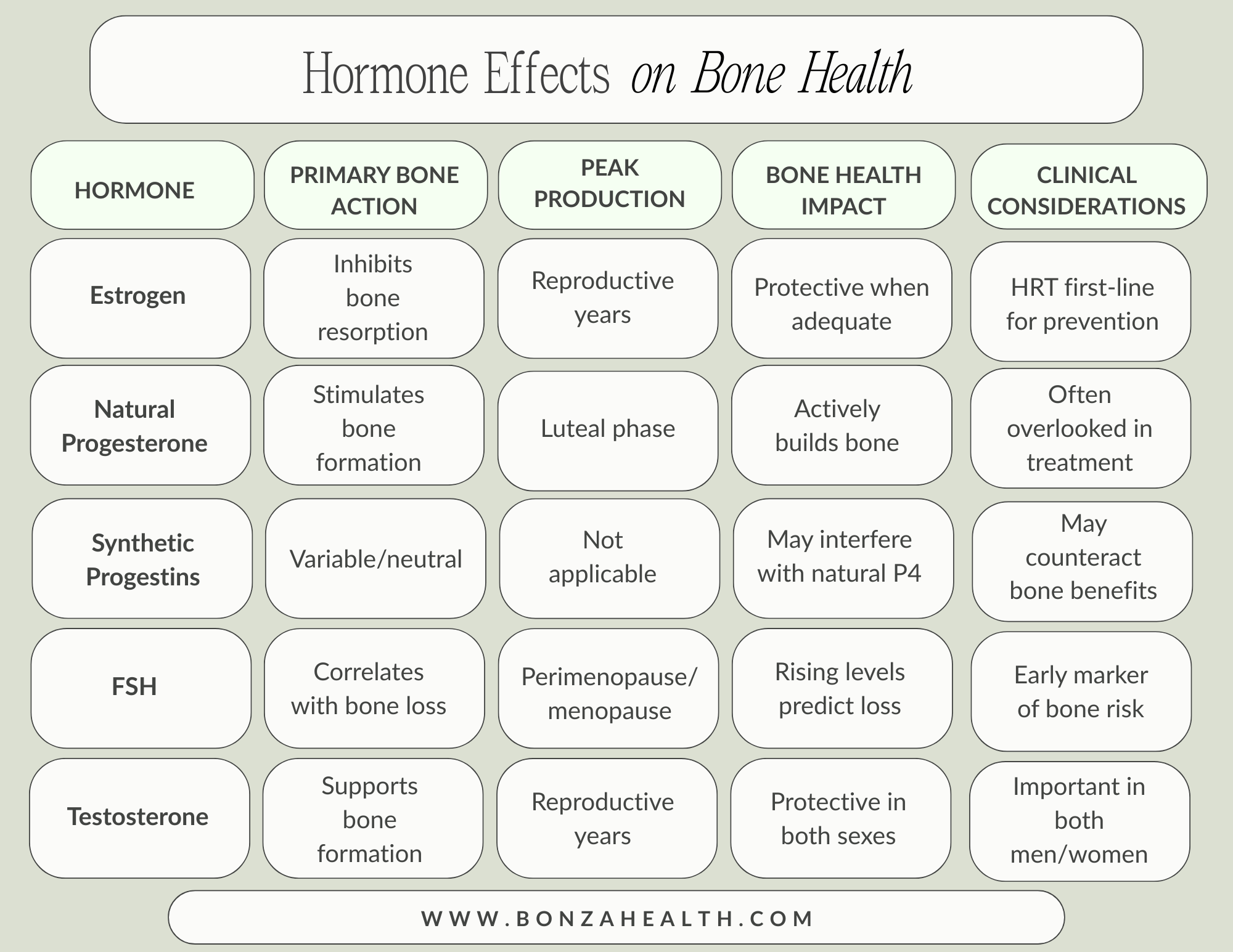
Estrogen serves as the body's primary bone protector, maintaining the delicate balance between bone formation and bone resorption. During the reproductive years, estrogen inhibits osteoclast activity—the cells responsible for breaking down bone tissue—while supporting osteoblast function for new bone formation.[5]
As estrogen levels fluctuate and ultimately decline during perimenopause, this protective mechanism fails.[4] The rapid bone loss phase begins when follicle-stimulating hormone (FSH) levels rise into the range of 34-56 IU/L, approximately two years before the final menstrual period.[1]
Interestingly, research shows that bone loss rates correlate more strongly with FSH levels than with estradiol concentrations, suggesting that the hormonal changes of perimenopause impact bone health even when estrogen levels appear normal.[3,6]
The Case for Earlier DEXA Screening
Current Guidelines Fall Short
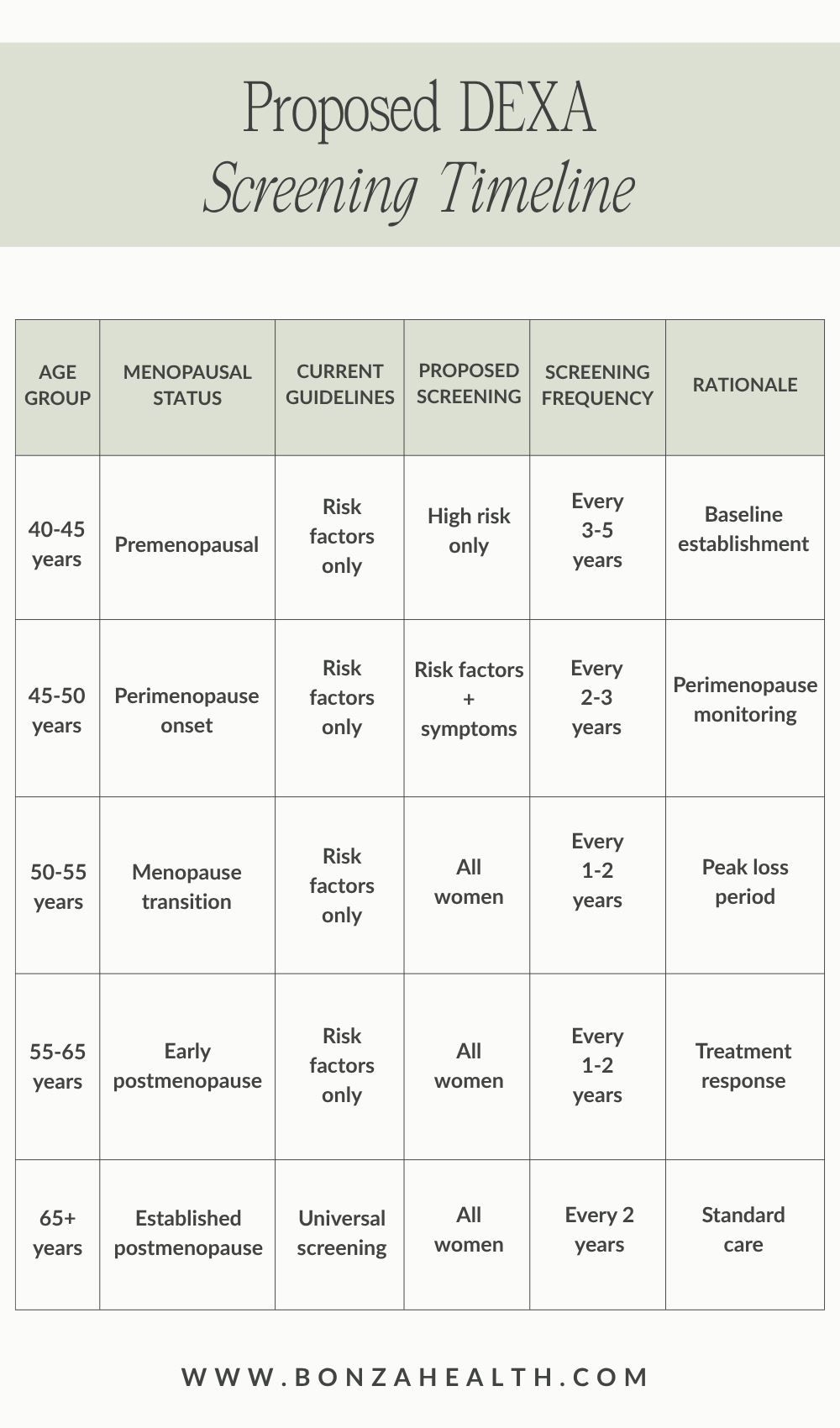
While current guidelines recommend routine DEXA screening for women aged 65 and older, with selective screening for younger women with specific risk factors, this approach may miss critical opportunities for intervention. The most rapid bone loss occurs during the perimenopausal transition—typically in a woman's late 40s to early 50s—yet screening often doesn't occur until 10-15 years later.[7]
A study of 714 asymptomatic perimenopausal women found that 47.6% already had osteopenia or osteoporosis, with 37.6% showing osteopenia and 10% demonstrating osteoporosis.[8] These findings suggest that significant bone loss is already occurring during the perimenopausal years, making early detection crucial for effective intervention.
The Preventive Medicine Approach
Early DEXA screening during perimenopause offers several compelling advantages:[9]
Early Detection and Intervention: Identifying bone loss during its most active phase allows for timely interventions to prevent further deterioration rather than attempting to reverse established osteoporosis.
Personalized Risk Assessment: Baseline bone density measurements during perimenopause provide crucial information for assessing individual fracture risk and guiding treatment decisions.
Lifestyle Modification Guidance: Early screening results can motivate women to implement bone-protective lifestyle changes when they can have the greatest impact.
Treatment Timing Optimization: Research suggests that hormone replacement therapy and other bone-protective treatments are most effective when initiated early in the menopausal transition.[10]

The Progesterone Advantage: Nature's Bone Builder
Beyond Estrogen: The Role of Progesterone
While estrogen receives most attention in discussions of menopause and bone health, progesterone plays an equally important but distinct role in maintaining skeletal integrity.[11-13] Unlike estrogen, which primarily prevents bone resorption, progesterone actively promotes bone formation through its effects on osteoblasts.[11,13,14]
Research demonstrates that progesterone stimulates osteoblast differentiation and activity in a dose-dependent manner, with optimal effects occurring at physiological luteal phase concentrations.[11] In vitro studies show that progesterone exposure leads to a 70% increase in alkaline phosphatase concentrations—a marker of bone formation—within seven days, and a 2.7-fold increase after 21 days.[11]
Clinical Evidence for Progesterone's Bone Benefits
Meta-analyses reveal striking differences in bone health outcomes between women with normal ovulation versus those with ovulatory disturbances.[12,13] Women with regular ovulatory cycles show an estimated 0.5% increase in bone mineral density per year, while those with anovulation or short luteal phases experience a 0.7% annual decrease.[13]
Studies of postmenopausal women receiving hormone replacement therapy demonstrate that the combination of estrogen plus progestogens results in greater bone density improvements than estrogen alone: 1.3% annual increase with unopposed estrogens versus 1.7% with combined therapy.[13]
Dr. John R. Lee's landmark research showed a 15% average increase in bone mineral density among postmenopausal women using transdermal progesterone cream over three years, contrasting sharply with the 5% decline in untreated women.[14,15]
The Oral Contraceptive Paradox
The relationship between oral contraceptives and bone health presents a concerning paradox that deserves careful consideration, particularly for women with existing bone health concerns.[16] While some studies suggest potential benefits, emerging research indicates that hormonal contraceptives may actually impair bone health, especially when used during the critical bone-building years of adolescence and young adulthood.[16]
Research from the Group Health Research Institute found that teenage women using oral contraceptives with 30-35 micrograms of estrogen for over two years exhibited approximately 1% less bone density gain at both spine and whole-body sites compared to non-users. Perhaps more concerning, these effects persisted 12-24 months after discontinuing the contraceptives.[16]
The mechanism appears related to the synthetic progestins used in oral contraceptives, which lack the bone-building properties of natural progesterone. While estrogen-containing contraceptives may have some bone-protective effects in older women, progestin-only formulations show no benefit for bone density.[17]
This suggests that the synthetic hormones in oral contraceptives may interfere with the natural progesterone-mediated bone formation that occurs during regular ovulatory cycles.
Implementing a Perimenopausal Bone Health Strategy
Identifying Candidates for Early Screening
Women entering perimenopause should be considered for early DEXA screening if they have additional risk factors beyond hormonal changes:[18]
Family history of osteoporosis or hip fracture
Personal history of fractures after age 50
Low body weight (BMI < 20) or significant weight loss
Use of glucocorticoids or other bone-affecting medications
Smoking or excessive alcohol consumption
Chronic diseases affecting bone health
Early or surgical menopause
History of prolonged amenorrhea or eating disorders
The Comprehensive Approach
Optimal bone health during perimenopause requires a multifaceted approach:[1,19]
Nutritional Support: Adequate calcium (1000-1200 mg daily) and vitamin D (800-1000 IU daily) intake forms the foundation of bone health.
Exercise Protocol: High-intensity resistance training and weight-bearing exercises specifically target bone formation and have been shown to improve bone density.
Hormone Optimization: Consider bioidentical hormone replacement therapy, including natural progesterone, for women with significant symptoms or early bone loss.[11,12]
Lifestyle Modifications: Smoking cessation, alcohol moderation, and fall prevention strategies reduce fracture risk.[1]
Supplement Considerations: Beyond calcium and vitamin D, nutrients like vitamin K2, magnesium, and boron support bone metabolism.[19]

The Economic and Health Case
Beyond Individual Health
The economic burden of osteoporotic fractures exceeds $19 billion annually in the United States, with costs projected to increase as the population ages.[20] Hip fractures alone carry a mortality rate of 20% within one year, making prevention strategies crucial not only for individual health but for public health outcomes.[19,20]
Early intervention during perimenopause offers the potential to prevent or delay the onset of osteoporosis, potentially reducing fracture rates and associated healthcare costs.[9] Studies suggest that women who maintain higher bone density entering menopause have significantly lower fracture risks throughout their later years.[21]
Recommendations for Clinical Practice
A Paradigm Shift in Bone Health
The evidence supports a fundamental shift in how we approach bone health screening for women. Rather than waiting until age 65, healthcare providers should consider implementing perimenopausal bone health assessments that include:
Baseline DEXA screening at menopause onset for all women, with earlier screening for those with risk factors.[7]
Comprehensive hormone evaluation including FSH, estradiol, and progesterone levels to assess ovulatory function.[3,13]
Lifestyle counseling focused on bone-protective behaviors during the critical perimenopausal window.[19]
Individualized treatment planning based on bone density results, fracture risk assessment, and hormonal status.[9]
Regular monitoring with follow-up DEXA scans every 1-2 years during active bone loss phases.[22]
Proactive Prevention Over Reactive Treatment
The perimenopausal transition represents a unique window of opportunity for bone health intervention that current medical guidelines largely ignore.[1,2] The evidence clearly demonstrates that the most significant bone loss occurs during this period, making it the optimal time for screening, assessment, and intervention.[2,3,6]
By shifting our focus from reactive treatment of established osteoporosis to proactive prevention during perimenopause, we can potentially prevent millions of women from experiencing the devastating consequences of osteoporotic fractures.[19,20] The integration of early DEXA screening with comprehensive hormone optimization—including attention to natural progesterone's bone-building effects—offers a promising approach to maintaining skeletal health throughout the menopausal transition and beyond.[11-13]
For women's health practitioners, the message is clear: bone health cannot wait until age 65. The battle for strong bones is won or lost during the perimenopausal years, making early screening and intervention not just beneficial, but essential for optimal long-term outcomes.[1,2]
The time has come to recognize perimenopause as the critical period it is for bone health and to adjust our screening and treatment paradigms accordingly.[2] By doing so, we can help ensure that women enter their later years with the strong, healthy bones they need to maintain independence, mobility, and quality of life.[19,20]

References
[1] Lo JC, Burnett-Bowie SA, Finkelstein JS. Bone and the perimenopause. Obstet Gynecol Clin North Am. 2011;38(3):503-517. doi:10.1016/j.ogc.2011.07.001
[2] Karlamangla AS, Burnett-Bowie SM, Crandall CJ. Bone health during the menopause transition and beyond. Obstet Gynecol Clin North Am. 2018;45(4):695-708. doi:10.1016/j.ogc.2018.07.012
[3] Neer RM; SWAN Investigators. Bone loss across the menopausal transition. Ann N Y Acad Sci. 2010;1192:66-71. doi:10.1111/j.1749-6632.2009.05233.x
[4] Endocrine Society."Menopause and Bone Loss | Endocrine Society." Endocrine.org, Endocrine Society, 16 June 2025, https://www.endocrine.org/patient-engagement/endocrine-library/menopause-and-bone-loss
[5] Kameda T, Mano H, Yuasa T, et al. Estrogen inhibits bone resorption by directly inducing apoptosis of the bone-resorbing osteoclasts. J Exp Med. 1997;186(4):489-495. doi:10.1084/jem.186.4.489
[6] Seifert-Klauss V, Fillenberg S, Schneider H, Luppa P, Mueller D, Kiechle M. Bone loss in premenopausal, perimenopausal and postmenopausal women: results of a prospective observational study over 9 years. Climacteric. 2012;15(5):433-440. doi:10.3109/13697137.2012.658110
[7] US Preventive Services Task Force, Nicholson WK, Silverstein M, et al. Screening for osteoporosis to prevent fractures: US preventive services task force recommendation statement. JAMA. 2025;333(6):498-508. doi:10.1001/jama.2024.27154
[8] Shariati-Sarabi Z, Rezaie HE, Milani N, Rezaie FE, Rezaie AE. Evaluation of bone mineral density in perimenopausal period. Arch Bone Jt Surg. 2018;6(1):57-62.
[9] Yong EL, Logan S. Menopausal osteoporosis: screening, prevention and treatment. Singapore Med J. 2021;62(4):159-166. doi:10.11622/smedj.2021036
[10] Nash Z, Al-Wattar BH, Davies M. Bone and heart health in menopause. Best Pract Res Clin Obstet Gynaecol. 2022;81:61-68. doi:10.1016/j.bpobgyn.2022.03.002
[11] Seifert-Klauss V, Prior JC. Progesterone and bone: actions promoting bone health in women. J Osteoporos. 2010;2010:845180. Published 2010 Oct 31. doi:10.4061/2010/845180
[12] Prior JC. Progesterone for the prevention and treatment of osteoporosis in women. Climacteric. 2018;21(4):366-374. doi:10.1080/13697137.2018.1467400
[13] Seifert-Klauss V, Schmidmayr M, Hobmaier E, Wimmer T. Progesterone and bone: a closer link than previously realized. Climacteric. 2012;15 Suppl 1:26-31. doi:10.3109/13697137.2012.669530
[14] Prior JC. Progesterone as a bone-trophic hormone. Endocr Rev. 1990;11(2):386-398. doi:10.1210/edrv-11-2-386
[15] Wellsprings Health. Osteoporosis and Natural Progesterone. Published 2022. Accessed June 16, 2025. https://www.wellsprings-health.com/pages/osteoporosis-and-natural-progesterone/
[16] HCPLive. Bone Density Reduction Observed in Some Birth Control Pill Users. Published July 20, 2011. Accessed June 16, 2025. https://www.hcplive.com/view/bone-density-reduction-observed-in-some-birth-control-pill-users
[17] Healthline. Can Birth Control Cause Bone Loss? Published October 9, 2025. Accessed June 16, 2025. https://www.healthline.com/health/birth-control-and-bone-loss
[18] Labcorp. Bone Mineral Density Screening. Accessed June 16, 2025. https://womenshealth.labcorp.com/providers/womens-health/bone-mineral-density-screening
[19] Rizzoli R, Bischoff-Ferrari H, Dawson-Hughes B, Weaver C. Nutrition and bone health in women after the menopause. Womens Health (Lond). 2014;10(6):599-608. doi:10.2217/whe.14.40
[20] de Villiers TJ. Bone health and menopause: Osteoporosis prevention and treatment. Best Pract Res Clin Endocrinol Metab. 2024;38(1):101782. doi:10.1016/j.beem.2023.101782
[21] Shieh A, Ruppert KM, Greendale GA, et al. Associations of age at menopause with postmenopausal bone mineral density and fracture risk in women. J Clin Endocrinol Metab. 2022;107(2):e561-e569. doi:10.1210/clinem/dgab690
[22] Stamford Health. What The Updated Osteoporosis Screening Guidelines Means For You. Published March 5, 2025. Accessed June 16, 2025. https://www.stamfordhealth.org/healthflash-blog/integrative-medicine/updated-osteoporosis-screening-guidelines/