
The Hidden Agony: Undiagnosed Endometriosis in Perimenopause
Written and edited by Sarah Bonza MD, MPH, MSCP, FAAFP, DipABLM, NBC-HWC

Many women with endometriosis experience bloating, constipation, diarrhea, and abdominal cramping.
I still remember the look on her face. She was in her early 40s, sitting on the edge of the exam table, clutching her abdomen and fighting back tears. “I’ve been to the ER three times this month,” she said. “Nobody can find anything wrong, but the pain is unbearable. They say it’s probably anxiety or IBS. Am I going crazy?”
If you’re reading this and nodding along, you are not alone. As a board-certified family physician and Menopause Society Certified Practitioner, I have met countless women in their late 30s and early 40s who have suffered for years with unexplained abdominal pain, only to be told, over and over, that “everything is fine.”
But for many of these women, the real culprit is undiagnosed endometriosis, a condition that can become especially troublesome during the hormonal rollercoaster of perimenopause.[1]
Today, I want to share what I’ve learned from my patients, the science, and my own clinical experience. If you or someone you love is struggling with mysterious pain, this story is for you.
What Is Endometriosis?
Let’s start with the basics. Endometriosis is a chronic, estrogen-dependent condition where tissue similar to the lining of the uterus (the endometrium) grows outside the uterus—on the ovaries, fallopian tubes, pelvic lining, and sometimes even the bowel or bladder. These patches of tissue, called ectopic endometrial tissue, act just like the uterine lining: they thicken, break down, and bleed in response to hormonal signals each month.
But unlike the normal uterine lining, this tissue has nowhere to go. The result? Chronic inflammation, pain, scarring, and sometimes infertility.
Endometriosis affects up to 10% of women of reproductive age, but it is still woefully underdiagnosed, especially in women approaching menopause.[2]

Endometriosis is a condition where tissue similar to the lining of the uterus (the endometrium) grows outside the uterus. It grows on the ovaries, fallopian tubes, pelvic lining, and sometimes even the bowel or bladder.
The Perimenopause Puzzle: Hormones in Flux
Perimenopause, the years leading up to menopause, is a time of profound hormonal change. Many women expect their estrogen and progesterone levels to gradually decline, but the reality is far more chaotic.
During perimenopause, estrogen levels can spike unpredictably, sometimes reaching higher peaks than in the regular menstrual cycle. Progesterone, meanwhile, may fall or fluctuate erratically.
These hormonal surges and dips can wreak havoc on a woman’s body. And for those with endometriosis, they can trigger painful flares.[3]
Why Do Estrogen Peaks Matter?
Estrogen is the fuel that drives endometriosis. It stimulates both the normal uterine lining and any ectopic endometrial tissue, causing them to grow and become inflamed. When estrogen levels surge, as they often do in perimenopause, undetected or residual endometrial tissue can become highly active, leading to sudden, severe pain.
I’ve seen women who made it through their 20s and 30s with only mild or manageable period pain, only to be blindsided by debilitating symptoms in their late 30s or 40s. For many, these symptoms are not cyclical anymore: They’re persistent, unpredictable, and often misdiagnosed as gastrointestinal or psychological problems.
The Overlap with IBS: A Diagnostic Trap
One of the most frustrating aspects of endometriosis is its tendency to mimic other conditions, especially irritable bowel syndrome (IBS). Many women with endometriosis experience bloating, constipation, diarrhea, and abdominal cramping. These symptoms overlap so much with IBS that it’s easy for both patients and providers to miss the real diagnosis.[4]
In fact, studies show that women with endometriosis are more likely to be diagnosed with IBS, and vice versa. This overlap leads to a cycle of misdiagnosis and dismissal, where women are told their pain is “all in their head” or due to stress.
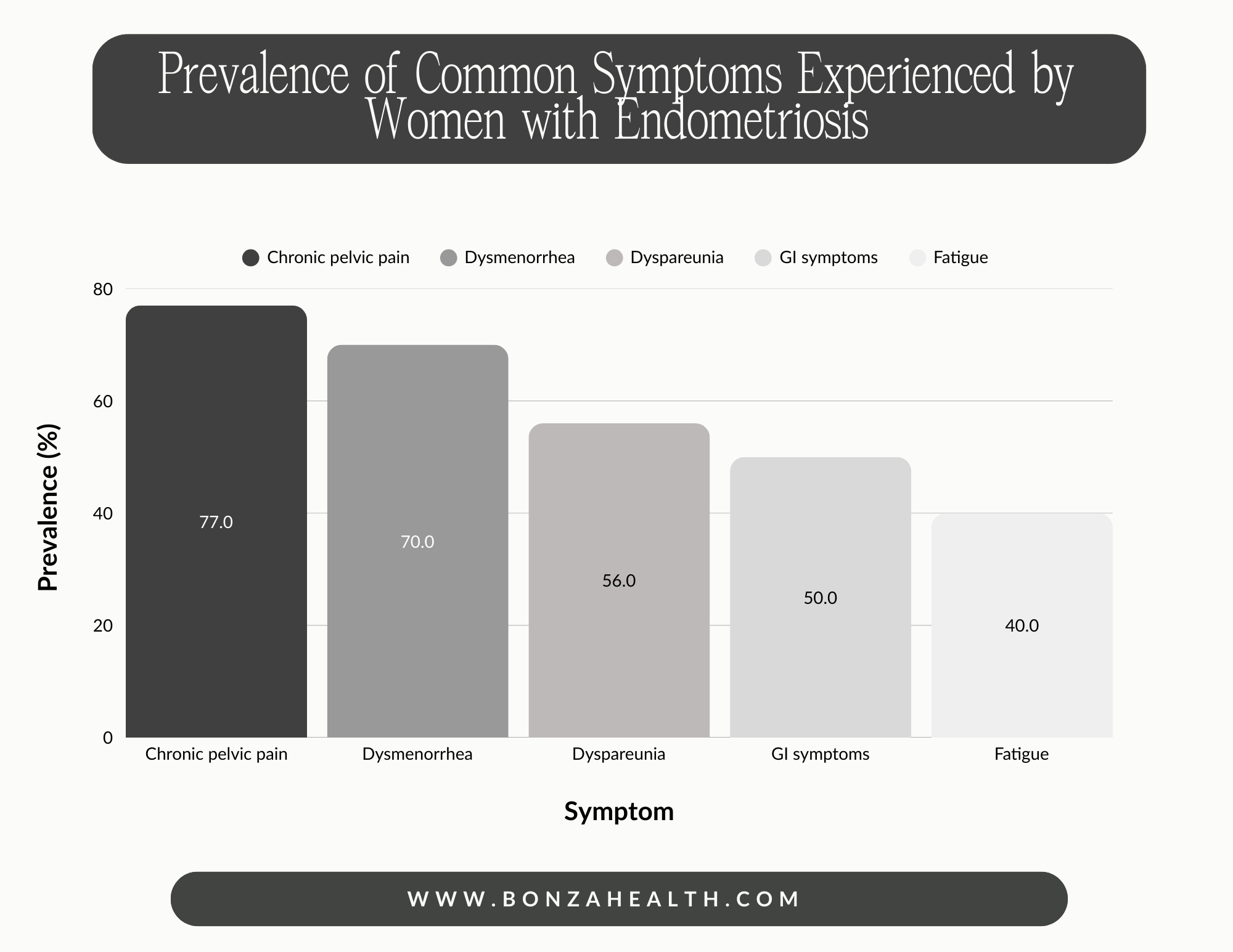
Chronic pelvic pain is the most common symptom among women with endometriosis.
The ER Merry-Go-Round: When Pain Becomes an Emergency
Let me share a story that’s all too common in my practice.
One of my patients, let’s call her Lisa, was a healthy, active woman in her late 30s. She had always had painful periods, but nothing she couldn’t handle. Then, seemingly out of nowhere, she began experiencing excruciating abdominal pain that would strike without warning.
The pain was so severe that she ended up in the emergency room multiple times. Each time, she underwent CT scans, blood tests, and even exploratory surgery. The results? “Everything looks normal.” She was sent home with painkillers and a referral to a gastroenterologist.
Lisa’s story is not unique. I’ve had several patients, women who are teachers, nurses, and business owners, who have been through this same cycle. They are told their pain is not real, or that it’s caused by anxiety, depression, or IBS. Some are even labeled as malingerers.
But the pain is real. And for many, it’s endometriosis.
How Perimenopause Triggers Endometriosis Flares
So why does perimenopause make things worse? The answer lies in the hormonal chaos of this stage of life.
During perimenopause, the ovaries become less predictable. Some months, they may produce very little estrogen; other months, they may produce surges of estrogen that are higher than anything seen in the regular menstrual cycle. These estrogen peaks can stimulate any remaining or undetected endometrial tissue, causing it to grow, bleed, and inflame the surrounding tissues.[5]
At the same time, progesterone levels often drop or become erratic. Progesterone normally acts as a “brake” on endometrial growth, counteracting the effects of estrogen. When progesterone is low or inconsistent, estrogen’s effects go unchecked, leading to flares of pain and inflammation.
This is why so many women experience their first severe symptoms of endometriosis in their late 30s or 40s, even if they never had a diagnosis before.
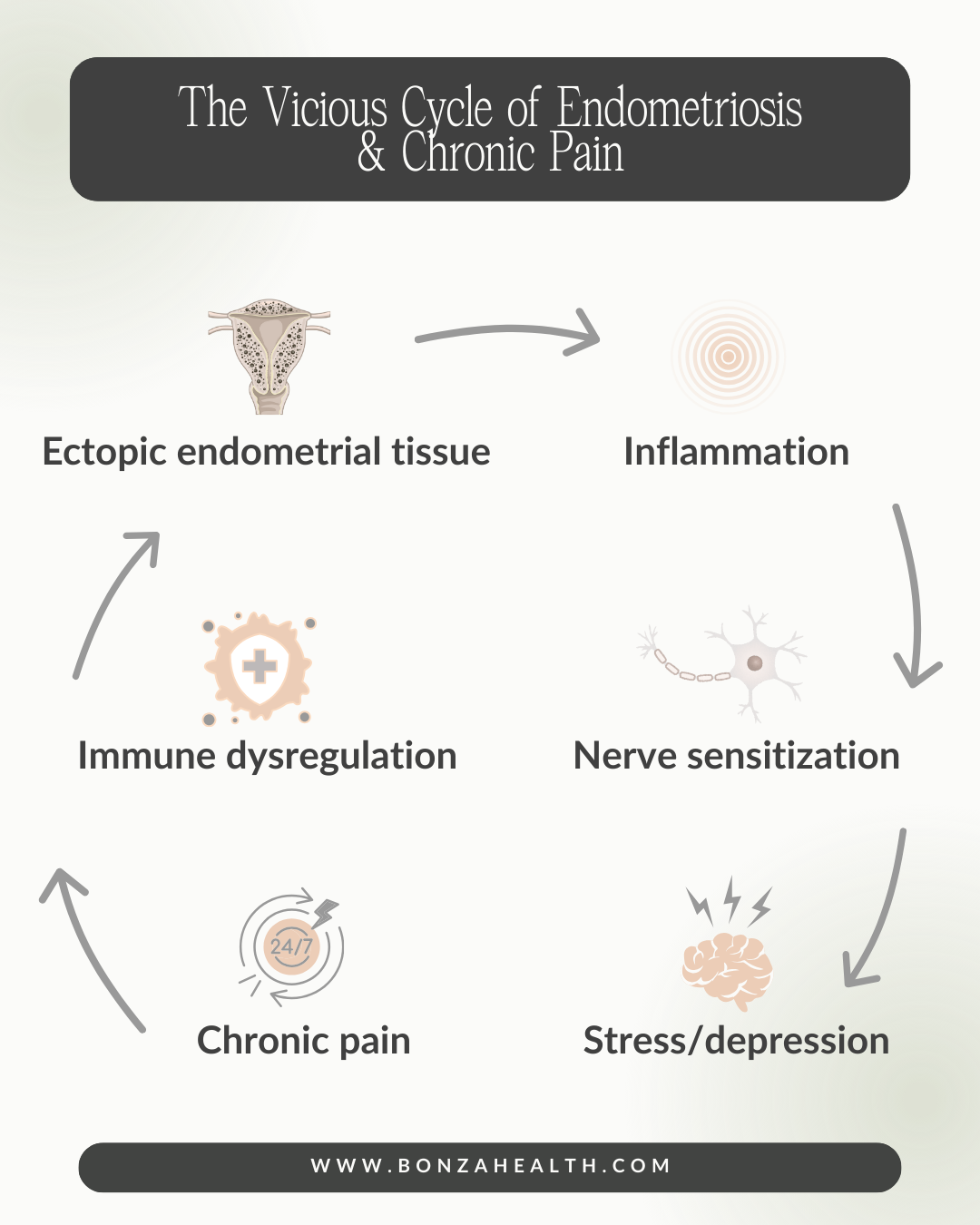
Endometriosis is a chronic, systemic, and inflammatory disease with a feedback loop involving pain, immune dysfunction, and psychological symptoms.
The Importance of Listening: My Approach at Bonza Health
When women come to my practice, Bonza Health, they are often at the end of their rope. They’ve been to multiple specialists, tried countless diets and medications, and still have no answers. My first job is to listen. I take a detailed history, paying special attention to:
Past and present menstrual symptoms
Abdominal and pelvic pain patterns
GI symptoms (bloating, constipation, diarrhea)
Triggers and timing of pain
Previous diagnoses and treatments
I also ask about their experiences with hormone therapy, birth control, and any surgeries (like hysterectomy or oophorectomy).

As a board-certified family physician and certified Menopause Society Practitioner, my first job is to listen to patients experiencing symptoms of endometriosis.
Hormonal Therapy: Why Progesterone Is Key
For women with endometriosis, hormonal therapy is the cornerstone of treatment. Because endometriosis is fueled by estrogen, the goal is to reduce estrogen’s effects and support the body with adequate progesterone. [6,7]
Progesterone: The Unsung Hero
Many of my patients with endometriosis feel dramatically better on higher doses of progesterone. Progesterone helps suppress the growth and activity of endometrial tissue, both inside and outside the uterus. It also has anti-inflammatory properties that can help reduce pain and swelling.
I’ve seen remarkable transformations in women who were started on progesterone after years of suffering. Two of my patients, both with multiple ER visits for severe pain, experienced substantial relief and a return to daily function once we initiated progesterone therapy. One told me, “I feel like I’m finally getting my life back.”
Caution with Estrogen: Less Is More
After surgical menopause (such as hysterectomy for endometriosis), some women are started on estrogen replacement therapy to manage hot flashes, night sweats, and other menopausal symptoms. However, high doses of estrogen, especially oral estrogen, can reactivate endometriosis or worsen symptoms.[8,9]
Let me share another story.
A patient in her late 30s, who had undergone a hysterectomy for endometriosis, was started on 2mg oral estrogen. Within weeks, she developed intractable nausea, vomiting, and severe abdominal pain. She was hospitalized for over a week, with mildly elevated pancreatic enzymes and a diagnosis of pancreatitis of unknown cause.
As her estrogen levels decreased, her pain improved. When we added progesterone to her regimen, she told me, “I feel like myself again.”

Progesterone helps suppress the growth and activity of endometrial tissue, both inside and outside the uterus. However, high doses of estrogen, especially oral estrogen, can reactivate endometriosis or worsen symptoms
Transdermal Estradiol: A Safer Option
Transdermal estradiol (applied as a patch, gel, or spray) is generally preferred over oral estrogen for women with endometriosis. It provides effective symptom relief with a lower risk of stimulating residual endometrial tissue and fewer systemic side effects.
The lowest effective dose should always be used, and progesterone must be included if there is any possibility of residual endometrial tissue.[10] I prescribe progesterone for these patients even if they have had a hysterectomy.
Oral Contraceptives vs. Menopausal Hormone Therapy
It’s important to note that oral contraceptives contain much higher doses of estrogen than typical menopausal hormone therapy. For women with endometriosis, this higher estrogen exposure can increase the risk of symptom recurrence or progression.[11]
Menopausal hormone therapy should use the lowest effective dose of transdermal estradiol, always combined with adequate progesterone.
Action Steps: What You Can Do
If you are a woman in your late 30s or 40s with a history of painful periods, unexplained abdominal pain, or IBS-like symptoms that have not responded to standard GI workups, consider endometriosis as a possible cause, especially if your pain worsens with hormonal fluctuations. Here’s what you can do:
Track Your Symptoms
Keep a diary of your pain, GI symptoms, and menstrual cycles. Note any patterns or triggers.
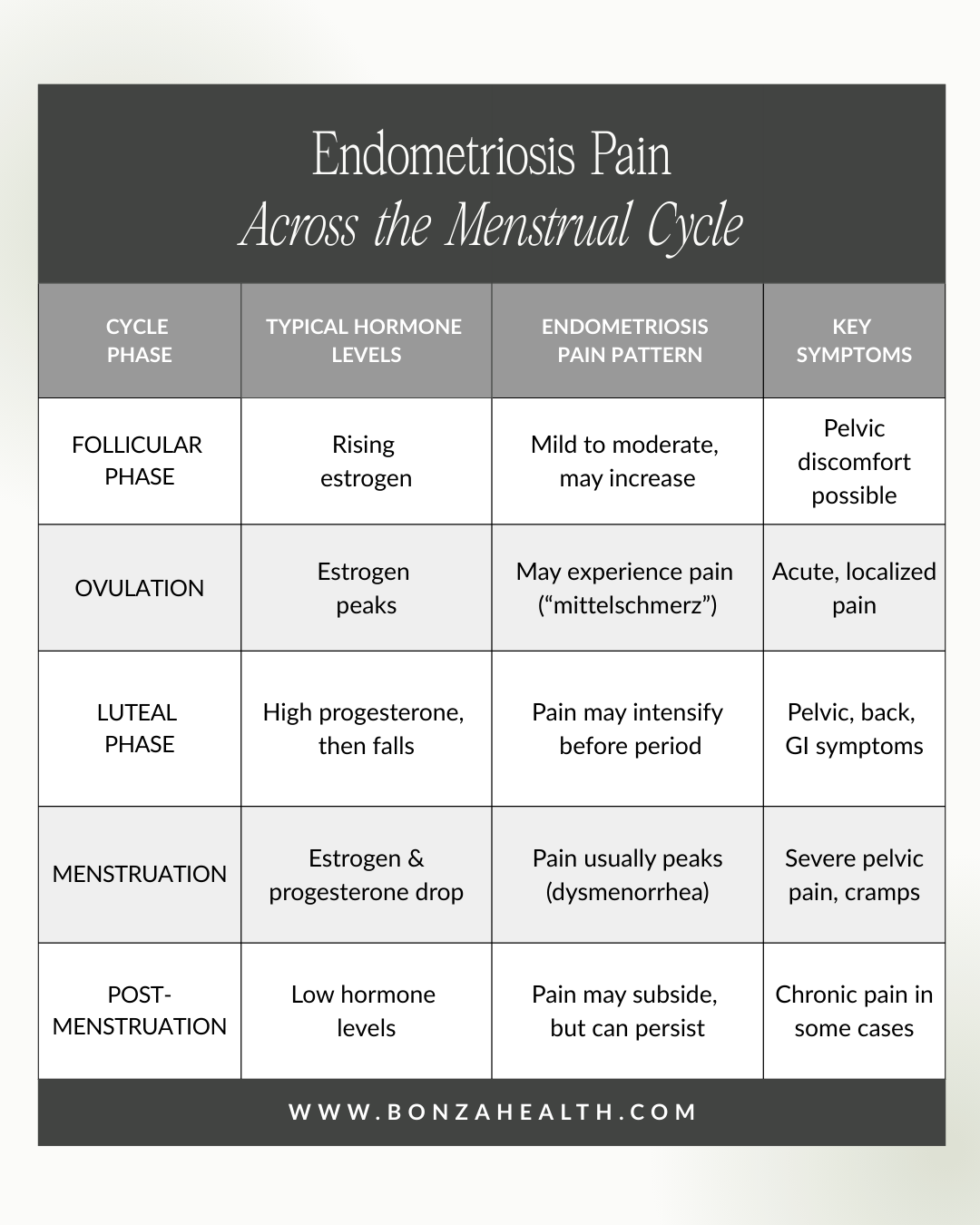
A typical pain pattern in endometriosis includes the following:
Endometriosis pain most commonly worsens during the days leading up to and during menstruation (late luteal phase and menstrual phase). This is known as dysmenorrhea and is a hallmark of the disease.
Many patients also report pain that begins the day before their period or mid-cycle (around ovulation in the follicular phase). However, the most intense pain is usually just before and during menstruation.
Over time, especially with chronic disease, pain can become chronic (present daily or most days) and less tied to the cycle: a phenomenon known as chronic pelvic pain or acyclical pain.
Hormonal fluctuations, particularly rising estrogen in the late follicular phase and the drop in progesterone before menstruation, can stimulate ectopic endometrial tissue, leading to inflammation and pain.
Endometriosis pain most commonly worsens during the days leading up to and during menstruation. Many patients also report pain that occurs mid-cycle (around ovulation in the follicular phase).
Advocate for Yourself
If you feel dismissed or unheard, seek a second opinion, preferably from a provider experienced in women’s health and menopause
Ask About Hormonal Therapy
Discuss the possibility of progesterone therapy or adjusting your current hormone regimen.
Consider Functional Testing
In some cases, additional testing may help uncover underlying inflammation or hormonal imbalances.
Prioritize Wellness
Focus on whole-food, plant-based nutrition, regular movement, stress management, and restorative sleep, all of which can help modulate inflammation and support hormonal balance.

A whole-food, plant-based diet is essential in the management of endometriosis.
You Are Not Alone
If you recognize yourself in this story, know that you are not alone, and you are not “crazy.” Your pain is real, and effective treatment is possible.
At Bonza Health, I am committed to helping women reclaim their vitality and find answers. If you’re ready to take the next step, I invite you to reach out. Together, we can unravel the mystery and chart a path toward healing.

For women with endometriosis, hormonal therapy is the cornerstone of treatment. The goal is to reduce estrogen’s effects and support the body with adequate progesterone.
References:
[1] E. Langmann, A.-C. Kainradl, M. Weßel, and A. Rokvity, Endometriosis in later life: an intersectional analysis from the perspective of epistemic injustice, Medicine Health Care and Philosophy, vol. 28, no. 1, p. 151, Dec. 2024. https://doi.org/10.1007/s11019-024-10245-4
[2] M.-D. Dinu et al., Endometriosis in Menopausal Women—A New Age Is Coming? Literature Review, Life, vol. 14, no. 4, p. 485, Apr. 2024. https://doi.org/10.3390/life14040485
[3] Your hormones and endometriosis explained. May 2024. Accessed: Jul. 05, 2025. https://www.spirehealthcare.com/health-hub/specialties/diabetes-glands-and-hormones/your-hormones-and-endometriosis-explained/
[4] M. Fiorillo et al., Inflammatory Bowel Disease and Endometriosis: Diagnosis and Clinical Characteristics, Biomedicines, vol. 12, no. 11. Multidisciplinary Digital Publishing Institute, p. 2521, Nov. 04, 2024. https://doi.org/10.3390/biomedicines12112521
[5] A. A. Hegazy, A new look at the theoretical causes of endometriosis: Narrative review, International Journal of Reproductive BioMedicine (IJRM). Shahid Sadoghi University of Medical Sciences of Yazd, Jul. 02, 2024. https://doi.org/10.18502/ijrm.v22i5.16433
[6] S. Mechsner, Endometriosis, an Ongoing Pain—Step-by-Step Treatment, Journal of Clinical Medicine, vol. 11, no. 2. Multidisciplinary Digital Publishing Institute, p. 467, Jan. 17, 2022. https://doi.org/10.3390/jcm11020467
[7] Endometriosis and Natural Progesterone. Apr. 2023. Accessed: Jul. 05, 2025. https://www.cemcor.ubc.ca/ask/endometriosis-and-natural-progesterone
[8] Endometriosis – management after menopause. Apr. 2020. Accessed: Jul. 05, 2025. https://www.menopause.org.au/hp/information-sheets/endometriosis-management-after-menopause
[9] I. Jakson, A. L. Hirschberg, and S. Gidlöf, Endometriosis and menopause—management strategies based on clinical scenarios, Acta Obstetricia Et Gynecologica Scandinavica, vol. 102, no. 10, p. 1323, Apr. 2023. https://doi.org/10.1111/aogs.14583
[10] S. Vannuccini, S. Clemenza, M. Rossi, and F. Petraglia, Hormonal treatments for endometriosis: The endocrine background, Reviews in Endocrine and Metabolic Disorders, vol. 23, no. 3. Springer Science+Business Media, p. 333, Aug. 17, 2021. https://doi.org/10.1007/s11154-021-09666-w
[11] M. Zanello et al., Hormonal Replacement Therapy in Menopausal Women with History of Endometriosis: A Review of Literature, Medicina, vol. 55, no. 8. Multidisciplinary Digital Publishing Institute, p. 477, Aug. 14, 2019. https://doi.org/10.3390/medicina55080477