
When Your Mind Feels Like a Stranger: The Neurobiology of Perimenopause and Mood
Written and edited by Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBCHWC

Woman in perimenopause contemplating changes
You have done everything right. You have raised children, built a career, held your family together through illness, loss, and the relentless demands of modern life. You have been the person who fixes things, who shows up, who handles what needs to be handled. And then, sometime in your late thirties or forties, something shifts.
Maybe it started with a sleepless night that turned into a sleepless month. Maybe it was the first time you snapped at your partner over something trivial, then sat in your car crying because you could not understand why you felt so angry. Maybe it was the creeping dread that settled into your chest for no discernible reason—an anxiety you had never experienced, even during the most difficult seasons of your life.
And so you went to your doctor, hoping for answers. Perhaps you were told you were stressed. Perhaps you were handed a prescription for an antidepressant and told to practice self-care. One of my patients was advised to microdose marijuana throughout the day to manage her new anxiety. Another was told that her rage—episodes that terrified her because they felt utterly foreign to who she knew herself to be—was simply a sign that she needed better coping mechanisms.
This is not a failure of resilience. This is not a character flaw. This is biology—temporary, treatable biology that deserves to be understood, not dismissed.

You may still be functional—getting to work, keeping your household running, showing up for the people who depend on you. But inside, you feel like someone else has taken up residence in your body.
This Is Not New Depression—This Is Hormonal Disruption
Research consistently demonstrates that the perimenopause transition significantly increases vulnerability to mood symptoms, even in women with no prior history of depression or anxiety. The Harvard Study of Moods and Cycles found that premenopausal women with no history of major depression were nearly twice as likely to develop depressive symptoms during perimenopause compared to women who remained premenopausal[1]. Studies estimate that between 20 and 40 percent of perimenopausal women experience clinically significant depressive symptoms—many for the first time in their lives[2].
What makes perimenopause particularly disorienting is that it does not look like classic depression. You may still be functional—getting to work, keeping your household running, showing up for the people who depend on you. But inside, you feel like someone else has taken up residence in your body. The joy you once felt feels muted. The patience you relied upon has evaporated. The sense of capability and groundedness that defined you for decades seems to have abandoned you.
This experience has a biological basis. Your brain has spent your reproductive years bathed in estrogen and progesterone—hormones that do far more than regulate your menstrual cycle. They are architects of your neurotransmitter systems, and when they begin their erratic decline, your brain chemistry responds.
Brain changes in perimenopause
The Calm You Lost: Progesterone, Allopregnanolone, and Your GABA System
Progesterone is often overlooked in conversations about menopause, which tend to focus on estrogen. But progesterone begins its decline earlier than estrogen—often years before periods become irregular—and its loss has profound neurological consequences.
Here is what is happening in your brain: Progesterone is metabolized into a compound called allopregnanolone, a neurosteroid that directly interacts with GABA-A receptors. GABA (gamma-aminobutyric acid) is your brain's primary inhibitory neurotransmitter—it acts as the braking system for neuronal activity, promoting calm, reducing anxiety, and facilitating restful sleep. When allopregnanolone binds to GABA-A receptors, it produces effects remarkably similar to benzodiazepine medications: it is anxiolytic (anti-anxiety), sedative, and mood-stabilizing.
Published research in journals including Psychoneuroendocrinology and the Journal of Neuroendocrinology has demonstrated that progesterone's anxiolytic effects are mediated primarily through this allopregnanolone-GABA pathway[3,4]. Studies in both animal models and human subjects show that when progesterone levels drop, GABA function becomes impaired. The result is an uptick in anxious thoughts, heightened stress sensitivity, difficulty falling and staying asleep, and—critically—the emergence of irritability and rage that seems to come from nowhere.
This is the neurobiological basis for the experience so many women describe: "I feel like I have no buffer anymore. Everything gets under my skin. I used to let things roll off me, and now I cannot." Your buffer was, in part, the calming influence of allopregnanolone on your GABA receptors. When progesterone declines, that buffer diminishes.
The fits of rage that frighten you—the moments when you find yourself screaming at your spouse or children over something minor, then feeling devastated by your own behavior—these are not evidence that you are becoming a bad person. They are evidence that your neurological calming system has been disrupted. This is a biological event, not a moral failure.

When estrogen levels decline, women may experience an increased vulnerability to depression.
The Joy You Cannot Find: Estrogen, Serotonin, and Dopamine
While progesterone's decline drives much of the anxiety and rage, estrogen's fluctuation and eventual decline affects another critical aspect of mood: the capacity for joy, motivation, and emotional resilience.
Estrogen has extensive influence on serotonergic function. Research published in Behavioural and Cognitive Neuroscience Reviews and confirmed by subsequent neuroimaging studies demonstrates that estrogen enhances the production of serotonin by increasing the enzyme tryptophan hydroxylase, slows serotonin's breakdown into inactive metabolites, decreases serotonin reuptake (leaving more available in the synapse), and increases the density and sensitivity of serotonin receptors—particularly 5-HT2A receptors in areas of the brain concerned with mood regulation, cognition, and emotional processing[5-7].
When estrogen levels decline, each of these processes weakens. The result is often a flattening of mood, a loss of the emotional color that once made life feel vivid and engaging, and an increased vulnerability to depression.
Estrogen also modulates the dopaminergic system. Dopamine is the neurotransmitter of motivation, reward, and drive—it is what makes you want to engage with life, pursue goals, and experience pleasure from accomplishment. Studies published in journals including Brain Research and Synapse have demonstrated estrogen's role in dopamine regulation, particularly in brain regions associated with reward and motivation[8]. When estrogen declines, dopaminergic signaling can become impaired, contributing to reduced motivation, feelings of anhedonia (inability to experience pleasure), and cognitive inflexibility.
This helps explain the common perimenopausal experience of looking at your life—a life that might objectively be quite good—and feeling nothing. The activities that once brought satisfaction feel hollow. The drive that propelled you through your career feels absent. This is not ingratitude or laziness. This is dopaminergic disruption secondary to hormonal change.
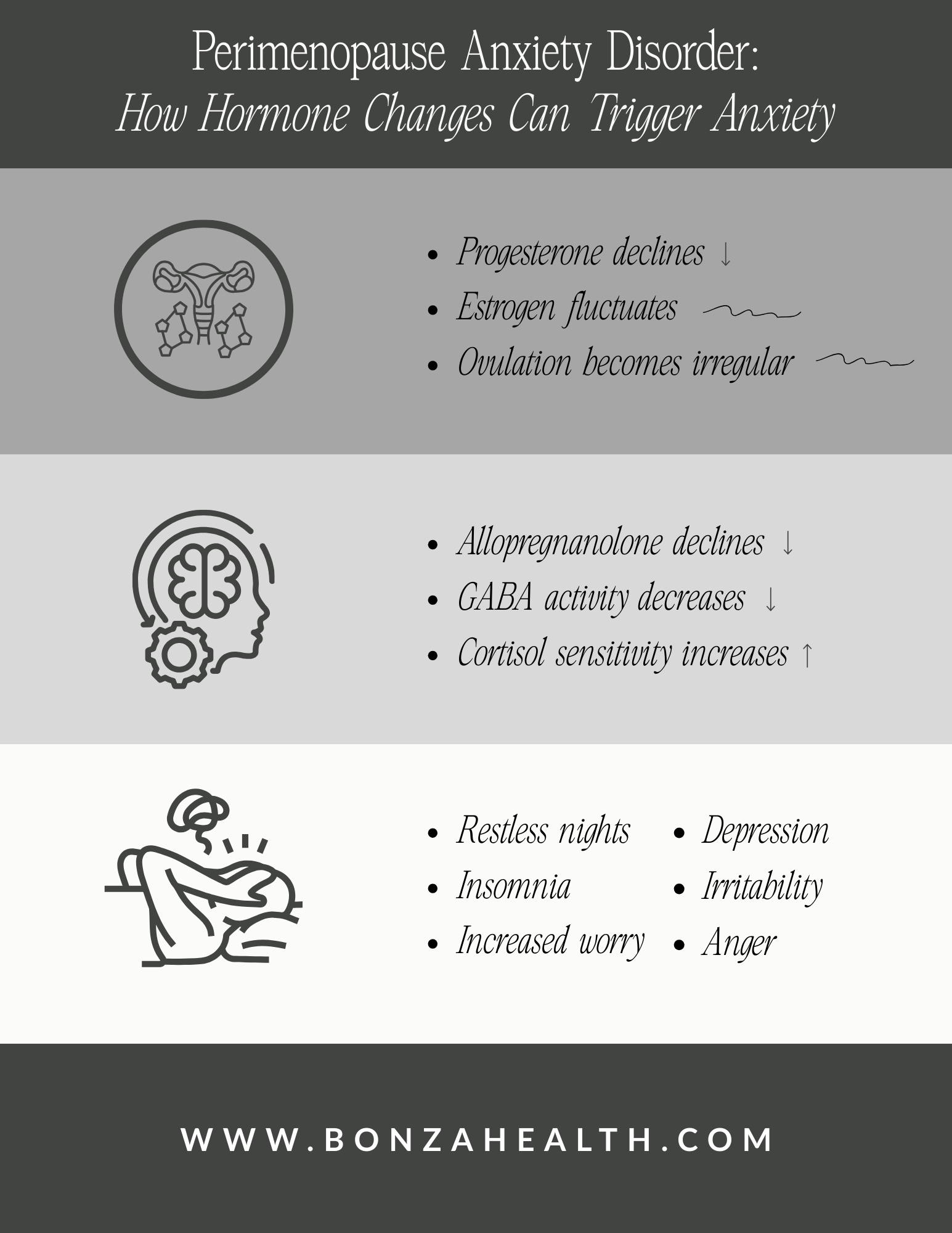
Image adapted from Dr. Jolene Brighten: https://drbrighten.com/perimenopause-anxiety-disorder
The Gut-Brain Axis: An Underrecognized Contributor
Approximately 90 percent of the body's serotonin is produced in the gut, not the brain. The connection between gut health and mood—mediated through what researchers call the gut-brain axis—has become a significant area of investigation in recent years.
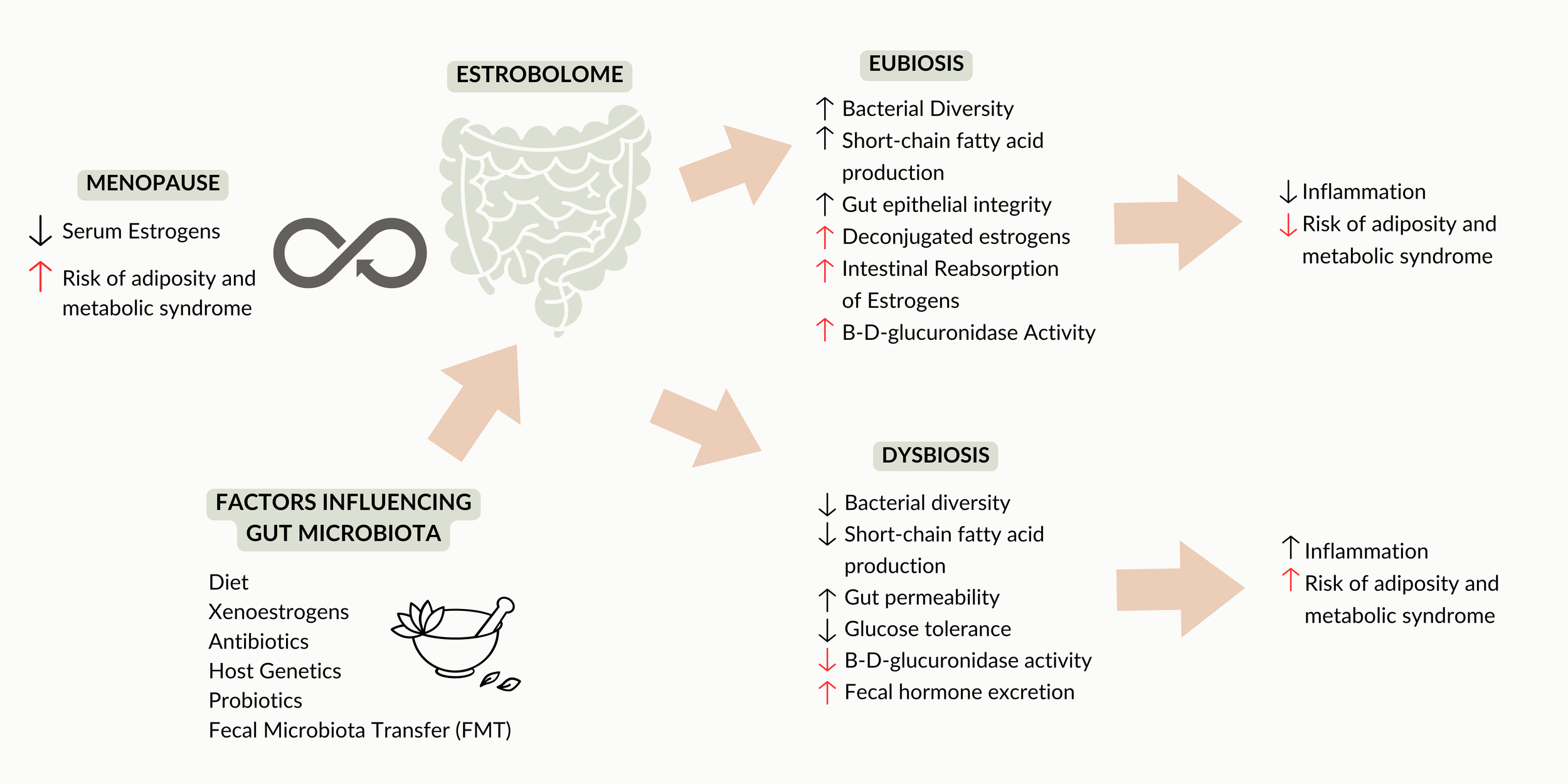
Estrogen influences the gut microbiome through what scientists have termed the "estrobolome"—the collection of gut bacterial genes capable of metabolizing estrogens. When estrogen levels fluctuate and decline during perimenopause, the composition and function of the gut microbiome can shift. This dysbiosis can affect the production of neuroactive substances, including GABA and serotonin, further contributing to mood symptoms[9,10].
This is one reason why addressing perimenopausal mood symptoms often requires a more comprehensive approach than simply prescribing an antidepressant. Gut health, nutrition, and the hormonal milieu all interact to influence brain chemistry.
Why This Matters: Beyond Individual Suffering
The impact of perimenopausal mood changes extends far beyond individual discomfort. These neurobiological shifts affect relationships, careers, and a woman's fundamental sense of self.
Marriages suffer when a partner's personality seems to change overnight. Children struggle to understand why their mother—who was once patient and available—now seems irritable and distant. Professional relationships fray when cognitive changes and mood instability affect performance. And perhaps most painfully, women lose trust in themselves, questioning their judgment, their capabilities, and their identity.
This is why understanding the biology matters. When you can explain to your husband that your brain's calming system has been disrupted by hormonal changes, when you can tell him that this is temporary and treatable rather than a fundamental change in who you are, it transforms the conversation. When you can communicate with your employer about cognitive changes that have a biological basis, you can advocate for support rather than suffering in silence and shame.

The impact of perimenopausal mood changes extends far beyond individual discomfort.
A Note to Medical Professionals
If you are a physician or healthcare provider reading this, I would ask you to consider: How many women in your practice are presenting with new-onset anxiety, depression, or mood lability in their late thirties and forties? How many have received prescriptions for SSRIs or anxiolytics without a discussion of hormonal contributors?
The 2019 clinical guidelines for the evaluation and treatment of perimenopausal depression, published in the Journal of Women's Health, explicitly recognize the menopausal transition as a window of vulnerability for mood disorders[11,12]. These guidelines emphasize the importance of considering hormone therapy as a treatment option, noting that estrogen therapy can be effective for depressive symptoms in perimenopausal women, particularly when initiated early in the menopausal transition.
The research is clear: mood symptoms in perimenopause often have a hormonal etiology and may respond to hormonal intervention. While antidepressants can certainly be helpful for some women, they do not address the underlying hormonal imbalance. A comprehensive approach—one that considers hormone therapy, lifestyle interventions, and targeted support for neurotransmitter function—often serves women better than psychiatric medication alone.

Hormone therapy can be an effective treatment option for depressive symptoms in perimenopausal women.
How to Advocate for Yourself
If you recognize yourself in this article and want to have a productive conversation with your healthcare provider, here is what I suggest:
First, connect your symptoms to your cycle and your age. Tell your doctor: "I am in my early forties (or late thirties, or late forties). These mood symptoms started around the same time my periods became irregular (or heavier, or more frequent). I have never experienced anxiety or depression like this before. I believe this may be related to perimenopause."
Second, ask specifically about hormonal evaluation and treatment. You might say: "I have read that progesterone affects the GABA system and can influence anxiety, and that estrogen affects serotonin production. Can we discuss whether hormone therapy might be appropriate for me, or whether my hormonal status should be evaluated?"
Third, if your provider dismisses these concerns or seems unfamiliar with the neurobiology of perimenopause, consider seeking a second opinion from a menopause specialist or a provider certified by The Menopause Society. You deserve care from someone who understands this transition.
There Is a Path Forward
What I have described in this article is not rare or unusual. It is a predictable consequence of hormonal change that I evaluate and treat routinely in my clinic. The neurobiology is well-established, and more importantly, it is actionable.
Menopause hormone therapy is not reserved for women who have completed the menopausal transition. It can be initiated during perimenopause—while you are still menstruating—to target the specific symptoms caused by progesterone and estrogen fluctuations. A physician trained in menopause care can assess your hormonal status, identify which neurotransmitter systems are most affected, and develop a personalized treatment protocol.
This might include progesterone to support GABA function and address anxiety, sleep disruption, and irritability. It might include estrogen to stabilize serotonin and dopamine systems. It will be tailored to you—your symptoms, your history, your life.
If your current provider is unfamiliar with this approach or has suggested that you simply need to wait it out, I encourage you to seek a consultation with a Menopause Society certified practitioner. Evidence-based treatment exists. You do not have to feel this way indefinitely.

Book your consult with Dr. Sarah Bonza, a Menopause Society-certified practitioner
References
[1] L. S. Cohen, C. N. Soares, A. F. Vitonis, M. W. Otto, and B. L. Harlow, “Risk for New Onset of Depression During the Menopausal Transition,” Archives of General Psychiatry, vol. 63, no. 4, p. 385, Apr. 2006, doi: 10.1001/archpsyc.63.4.385.
[2] E. W. Freeman, “Depression in the menopause transition: risks in the changing hormone milieu as observed in the general population,” Women s Midlife Health, vol. 1, no. 1. BioMed Central, Jul. 16, 2015. doi: 10.1186/s40695-015-0002-y.
[3] D. Bitran, R. H. Purdy, and C. K. Kellog, “Anxiolytic effect of progesterone is associated with increases in cortical alloprenanolone and GABAA receptor function,” Pharmacology Biochemistry and Behavior, vol. 45, no. 2, p. 423, Jun. 1993, doi: 10.1016/0091-3057(93)90260-z.
[4] D. Bitran, M. Shiekh, and M. K. McLeod, “Anxiolytic Effect of Progesterone is Mediated by the Neurosteroid Allopregnanolone at Brain GABAA Receptors,” Journal of Neuroendocrinology, vol. 7, no. 3, p. 171, Mar. 1995, doi: 10.1111/j.1365-2826.1995.tb00744.x.
[5] P. C. Bendis, S. Zimmerman, A. Onisiforou, P. Zanos, and P. Georgiou, “The impact of estradiol on serotonin, glutamate, and dopamine systems,” Frontiers in Neuroscience, vol. 18, Mar. 2024, doi: 10.3389/fnins.2024.1348551.
[6] L. A. Rybaczyk, M. J. Bashaw, D. R. Pathak, S. M. Moody, R. M. Gilders, and D. L. Holzschu, “An overlooked connection: serotonergic mediation of estrogen-related physiology and pathology,” BMC Women s Health, vol. 5, no. 1, Dec. 2005, doi: 10.1186/1472-6874-5-12.
[7] Z. Amin, T. Canli, and C. N. Epperson, “Effect of Estrogen-Serotonin Interactions on Mood and Cognition,” Behavioral and Cognitive Neuroscience Reviews, vol. 4, no. 1. SAGE Publishing, p. 43, Mar. 01, 2005. doi: 10.1177/1534582305277152.
[8] K. E. Yoest, J. Cummings, and J. B. Becker, “Estradiol, Dopamine and Motivation,” Central Nervous System Agents in Medicinal Chemistry, vol. 14, no. 2. Bentham Science Publishers, p. 83, Jan. 13, 2015. doi: 10.2174/1871524914666141226103135.
[9] W. Zhang et al., “Estradiol metabolism by gut microbiota in women’s depression pathogenesis: inspiration from nature,” Frontiers in Psychiatry, vol. 16. Frontiers Media, Jan. 28, 2025. doi: 10.3389/fpsyt.2025.1505991.
[10] H. Wang et al., “Gut microbiota has the potential to improve health of menopausal women by regulating estrogen,” Frontiers in Endocrinology, vol. 16. Frontiers Media, Jun. 09, 2025. doi: 10.3389/fendo.2025.1562332.
[11] H. D. Nelson, “Menopause,” The Lancet, vol. 371, no. 9614. Elsevier BV, p. 760, Mar. 01, 2008. doi: 10.1016/s0140-6736(08)60346-3.
[12] P. M. Maki et al., “Guidelines for the Evaluation and Treatment of Perimenopausal Depression: Summary and Recommendations,” Journal of Women s Health, vol. 28, no. 2. Mary Ann Liebert, Inc., p. 117, Sep. 05, 2018. doi: 10.1089/jwh.2018.27099.mensocrec.