
Why You Struggle to Burn Fat in Menopause (Even If You Lift Weights)
Written and edited by Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Why you struggle to burn fat in menopause (even if you lift weights)
You are doing everything "right." You are hitting the gym, prioritizing heavy lifting, and eating cleanly. In your 30s, this routine would have melted fat off your frame in a matter of weeks.
But now, in your 50s? The scale won't budge. You look in the mirror and see changes in your body composition—specifically around your midsection—that seem immune to your best efforts.
You feel "metabolically stuck."
I am here to tell you two things:
You are not imagining it.
It is not a lack of willpower.
Gaslighting yourself into thinking you just need to "try harder" or "eat less" is not the answer. The answer lies in understanding that your physiology has fundamentally shifted.

Drops in estrogen do far more than trigger hot flashes. It also flips a switch in your metabolic engine.
The Science: Estrogen Is a Metabolic Hormone
We tend to think of estrogen solely as a reproductive hormone—the thing that gives us periods and helps us make babies. But estrogen is actually a powerhouse metabolic regulator. It dictates how your body burns energy, where it stores fat, and how it responds to insulin [1].
During the transition into menopause, your ovaries stop producing consistent levels of estradiol. This drop does far more than trigger hot flashes; it flips a switch in your metabolic engine.
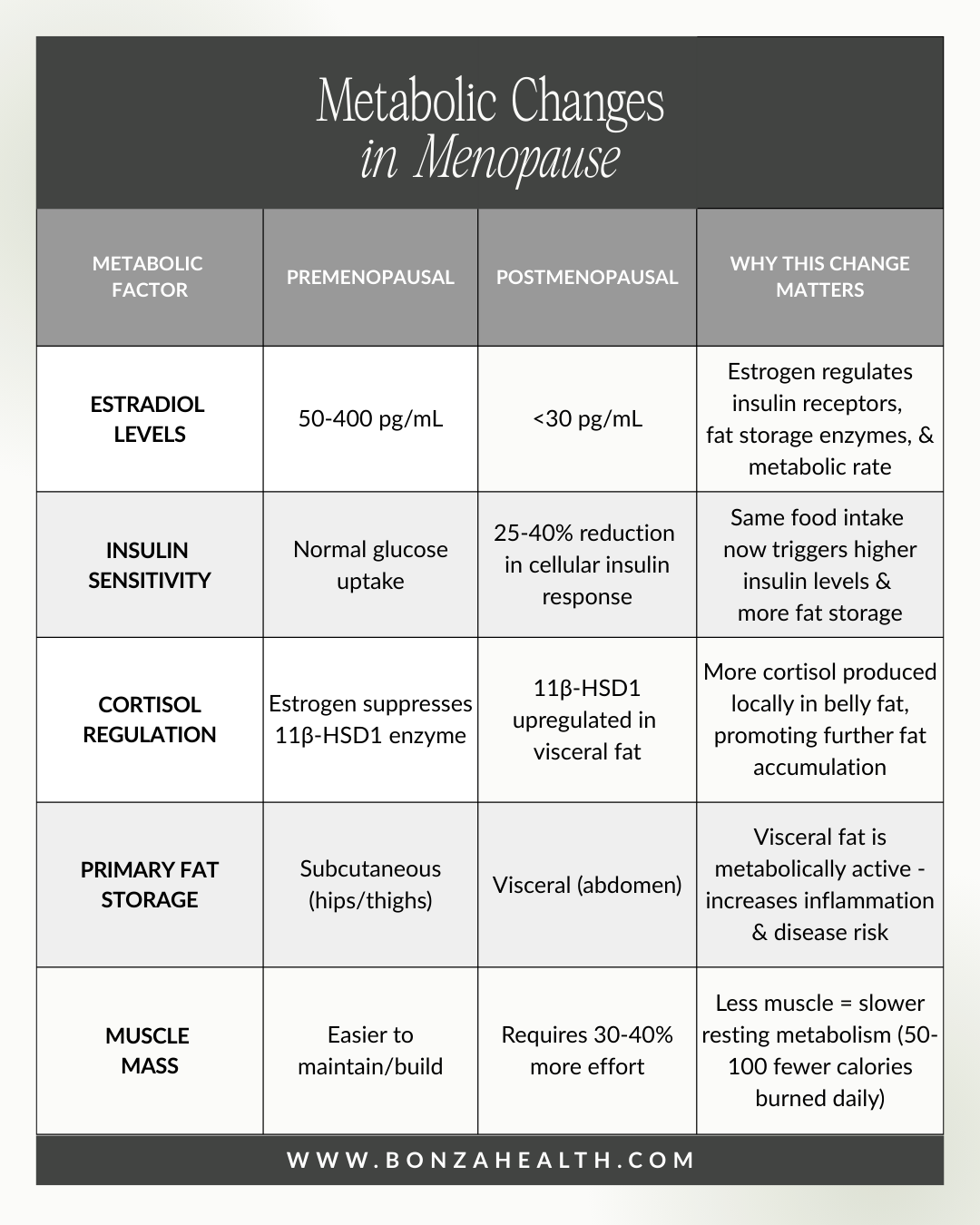
Metabolic changes in menopause
1. Insulin Sensitivity Drops
When you have abundant estrogen, your cells are "sensitive" to insulin—they easily open up to let glucose (sugar) in to be burned for energy. Research demonstrates that premenopausal women exhibit enhanced insulin sensitivity compared with age-matched men, but this advantage disappears after menopause due to a reduction in circulating estradiol [2].
As estrogen declines, your cells become resistant. Instead of burning glucose for fuel during your workouts, your body keeps that sugar circulating in the blood, where it eventually gets signaled to be stored as fat. Studies show that menopausal women are at greater risk of insulin resistance as estrogen levels fall during the menopause transition, with the body becoming less responsive to insulin [1,3].
You can be eating the exact same diet as you did ten years ago, but your body is now processing those calories differently. This shift in insulin sensitivity is not merely theoretical—research has demonstrated that declining estrogen levels significantly impact glucose homeostasis and insulin resistance in postmenopausal women [1,3].
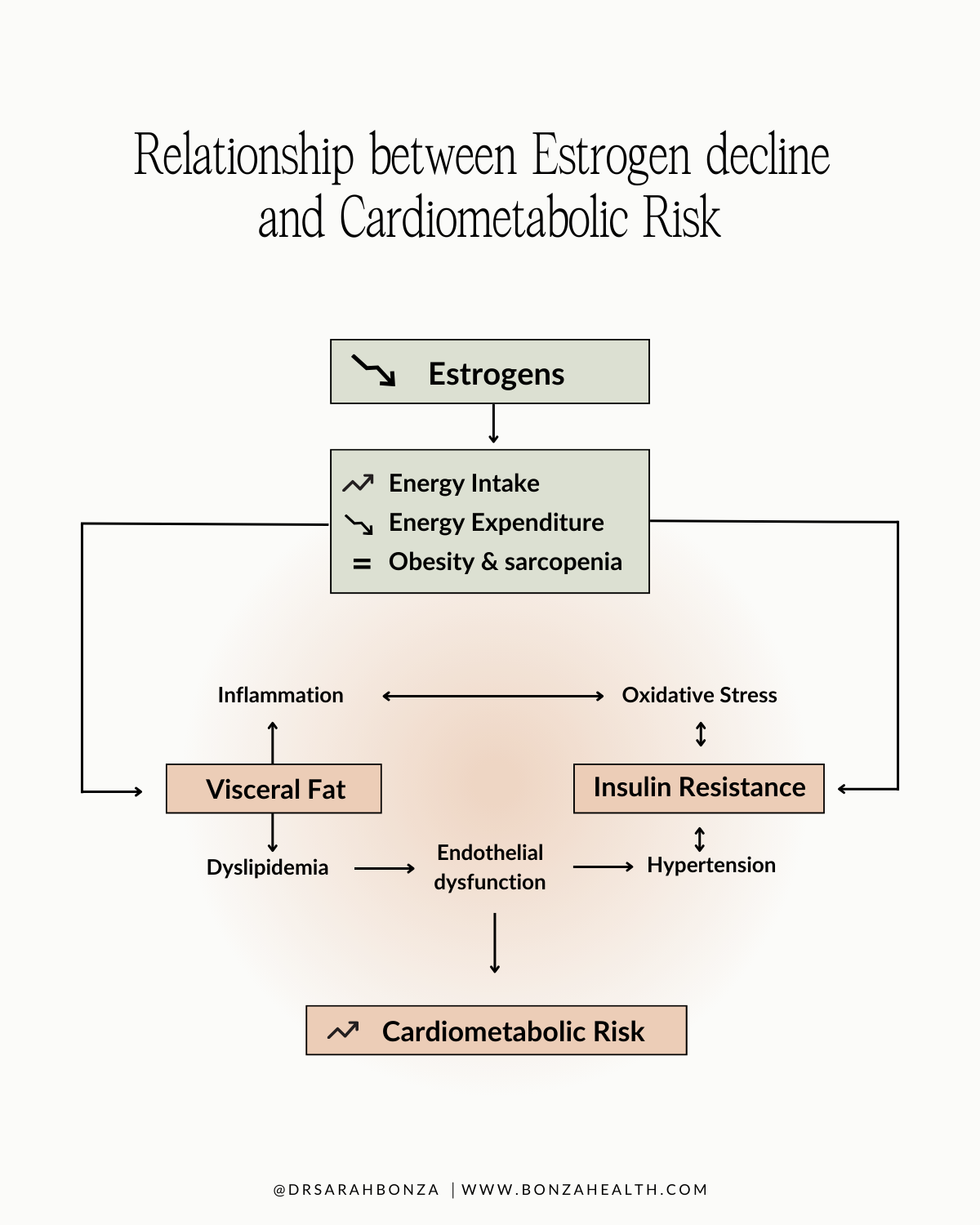
The relationship between estrogen decline and cardiometabolic risk.
2. The Cortisol "Belly" Effect
In menopause, we often see a relative "dominance" of cortisol effects, our primary stress hormone. Estrogen helps buffer the impact of cortisol through regulation of the enzyme 11β-HSD1, which converts inactive cortisone to active cortisol [4]. When estrogen declines, this enzyme becomes upregulated, particularly in visceral fat tissue in postmenopausal compared with premenopausal women [4].
High cortisol levels specifically encourage the storage of visceral fat—that stubborn deep belly fat that wraps around your organs. Research has consistently shown that women with higher cortisol levels demonstrate greater visceral fat accumulation, independent of total body weight [5]. During the menopausal transition, elevated cortisol levels promote visceral fat accumulation.
Moreover, chronic elevation of cortisol is catabolic, meaning it can break down muscle tissue. So you are fighting a battle on two fronts: your hormones are encouraging fat storage in the abdomen and potentially compromising the muscle you are working so hard to build in the gym.
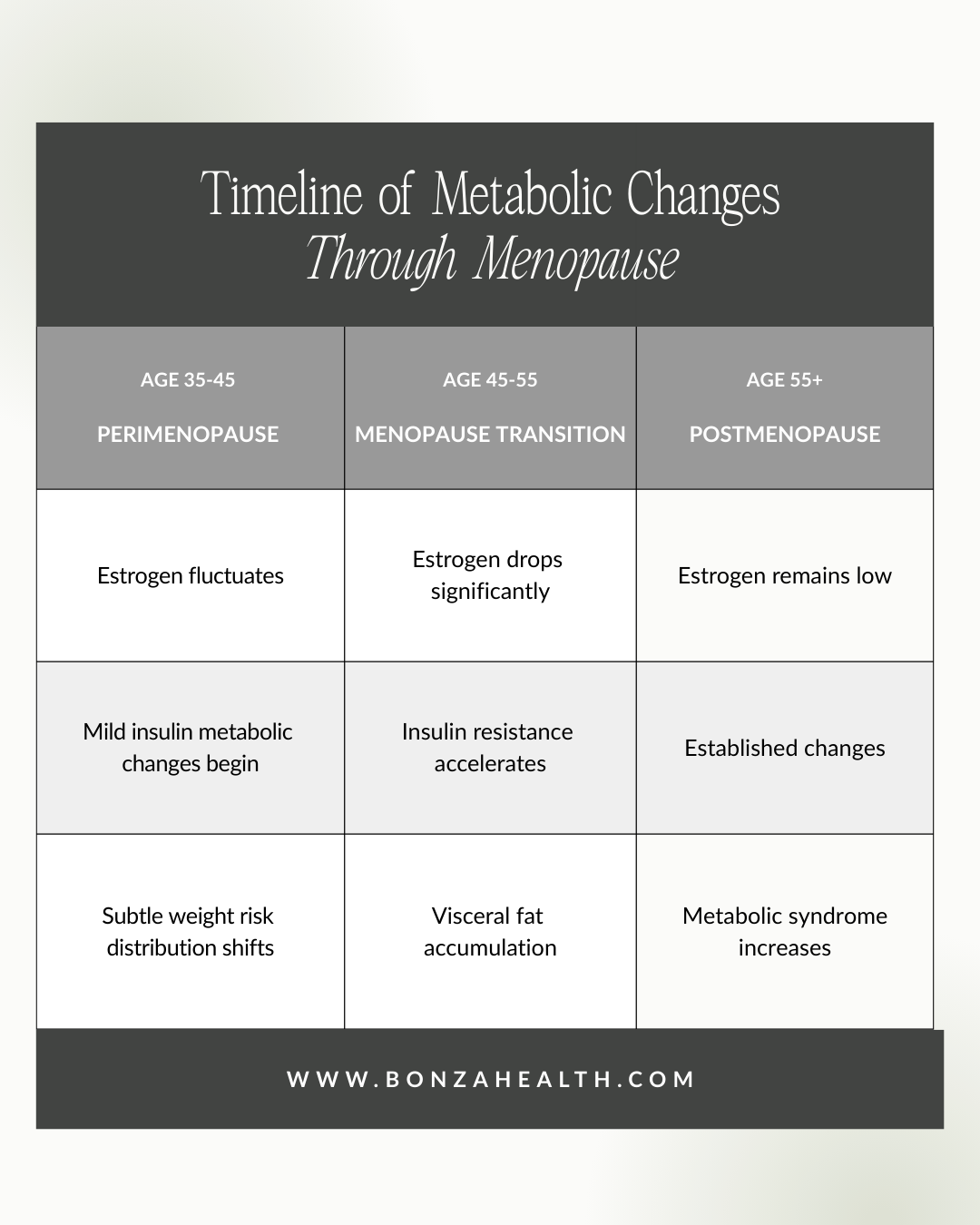
Timeline of metabolic changes through menopause
The Solution: A Precision Medicine Approach
If you feel like your metabolism has hit a wall, standard "eat less, move more" advice will likely fail you. In fact, over-restricting calories can spike cortisol further, making the problem worse.
We need to stop fighting your body and start supporting it. Here is the approach I use with my patients:
Hormone Optimization
This is the foundation. By restoring physiological levels of estradiol, we can help restore insulin sensitivity. Research has demonstrated that hormone therapy—including both oral and transdermal routes—can significantly reduce insulin resistance in healthy postmenopausal women [1,3].
Transdermal estradiol delivery (such as patches) is often preferred as it bypasses hepatic first-pass metabolism, potentially offering metabolic benefits with a different safety profile than oral formulations [6]. When estrogen levels are optimized through hormone therapy, research shows the body can begin responding to exercise more effectively by improving insulin sensitivity [7].
Important note: Hormone replacement therapy is not appropriate for everyone and should only be initiated after comprehensive evaluation with a qualified healthcare provider who can assess your individual risk factors and health history.

By restoring physiological levels of estradiol, we can help restore insulin sensitivity.
Metabolic Sensitizers: An Adjunctive Approach
Sometimes, hormones alone may not be sufficient to reverse years of metabolic adaptation. In select cases, metabolic sensitizers like metformin may be considered as adjunctive therapy.
While FDA-approved for type 2 diabetes, metformin has been studied for off-label use in non-diabetic populations. The Diabetes Prevention Program trial demonstrated that metformin produced modest but sustained weight loss (average 2.5 kg over 10 years) in participants with prediabetes, with particular effectiveness in subgroups including those with higher BMI and women with a history of gestational diabetes [8]. More recent research specifically examining perimenopausal women with prediabetes suggests that metformin may help manage metabolic changes during this transition through multiple mechanisms including improved insulin sensitivity and reduced inflammation [9].
It's important to understand that metformin is not specifically approved for weight management in healthy individuals, and evidence for its use in this context remains limited. Studies show modest weight loss effects (typically 2-5 kg), and it works best when combined with lifestyle modifications [8]. Any use of metformin for metabolic support in non-diabetic individuals represents off-label prescribing and should only be considered under close medical supervision with appropriate monitoring of blood glucose and vitamin B12 levels.
Metformin is not suitable for everyone and can have side effects, most commonly gastrointestinal symptoms. Long-term use may affect vitamin B12 absorption, requiring supplementation and monitoring.

In select cases, metabolic sensitizers like metformin may be considered as adjunctive therapy.
Let's Look Under the Hood
You do not have to accept "metabolic stuckness" as your new normal. If you are lifting heavy and showing up for yourself, your metabolism should show up for you—but it may need support to do so.
The Next Step
Stop guessing. Schedule a comprehensive consultation to evaluate your hormone levels and metabolic markers (including fasting glucose, insulin, hemoglobin A1c, and when indicated, cortisol patterns). Together, we can build a precision plan that supports your hard work in the gym.
Remember: the metabolic changes of menopause are real, scientifically documented, and treatable. You're not failing—your body's biochemistry has changed, and the solution lies in understanding and addressing those changes with evidence-based interventions tailored to your individual needs.

Are you a candidate for hormone therapy? Book a consult with Dr. Sarah Bonza.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. The information provided should not be used for diagnosing or treating a health problem or disease. Always consult with your healthcare provider before making any healthcare decisions or for guidance about a specific medical condition. Individual results may vary. Hormone replacement therapy and metformin are prescription medications that require medical evaluation and monitoring.
References
[1] M. De Paoli, A. Zakharia, and G. H. Werstuck, "The role of estrogen in insulin resistance: A review of clinical and preclinical data," Am. J. Pathol., vol. 191, no. 9, pp. 1490–1498, Sep. 2021. DOI: 10.1016/j.ajpath.2021.05.011
[2] H. Yan et al., "Estrogen improves insulin sensitivity and suppresses gluconeogenesis via the transcription factor Foxo1," Diabetes, vol. 68, no. 2, pp. 291–304, Feb. 2019. DOI: 10.2337/db18-0638
[3] K. Yasui et al., "Associations of estrogen and testosterone with insulin resistance in pre- and postmenopausal women with and without hormone therapy," Int. J. Endocrinol. Metab., vol. 11, no. 2, pp. 65–70, 2013. DOI: https://doi.org/10.5812/ijem.5333.
[4] H. Yamatani et al., "Association of estrogen with glucocorticoid levels in visceral fat in postmenopausal women," Menopause, vol. 20, no. 4, pp. 437–442, Apr. 2013. DOI: 10.1097/gme.0b013e318271a640
[5] E. S. Epel et al., "Stress may add bite to appetite in women: A laboratory study of stress-induced cortisol and eating behavior," Psychoneuroendocrinology, vol. 26, no. 1, pp. 37–49, Jan. 2001. DOI: 10.1016/s0306-4530(00)00035-4
[6] S. Vehkavaara et al., "Effect of estrogen replacement therapy on insulin sensitivity of glucose metabolism and preresistance and resistance vessel function in healthy postmenopausal women," J. Clin. Endocrinol. Metab., vol. 85, no. 12, pp. 4663–4670, Dec. 2000. DOI: 10.1210/jcem.85.12.7034
[7] A. S. Ryan, B. J. Nicklas, and D. M. Berman, "Hormone replacement therapy, insulin sensitivity, and abdominal obesity in postmenopausal women," Diabetes Care, vol. 25, no. 1, pp. 127–133, Jan. 2002. DOI: 10.2337/diacare.25.1.127
[8] Diabetes Prevention Program Research Group, "Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: The Diabetes Prevention Program Outcomes Study," Lancet Diabetes Endocrinol., vol. 3, no. 11, pp. 866–875, Nov. 2015. DOI: 10.1016/S2213-8587(15)00291-0
[9] B. S. Y. Lim, M. Chen, H.-Y. Li, and L.-J. Li, "Metformin use in prediabetes: A review of evidence and a focus on metabolic features among peri-menopausal women," Diabetes Obes. Metab., vol. 27, Suppl. 3, pp. 3–15, Jun. 2025. DOI: 10.1111/dom.16442