
The Progesterone Conversation Most Women Never Get to Have
Written and edited by Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Oral micronized progesterone is the FDA-approved, bioidentical form of progesterone that your body recognizes because it's structurally identical to what you've always made.
I've been practicing medicine for over two decades. I've sat with women in clinic, on hospital floors, and now through telehealth — and I can tell you that one of the most common moments I witness is this: a woman describes months of fragmented sleep, hot flashes at 2 a.m., anxiety that arrived out of nowhere, a fog that won't lift — and then adds, almost apologetically, "But I'm afraid of hormones."
That fear is real, and it didn't come from nowhere. It came from a 2002 study that made headlines around the world and led millions of women to stop — or never start — hormone therapy. What those headlines missed, and what took two more decades of research to fully untangle, is that not all hormones behave the same way in your body. The type matters enormously.
One of the most important distinctions in menopausal medicine right now is the difference between oral micronized progesterone — the FDA-approved, bioidentical form that your body recognizes because it's structurally identical to what you've always made — and the older synthetic progestins like medroxyprogesterone acetate (MPA) that were used in those early studies. These are not interchangeable molecules. They bind to receptors differently, metabolize differently, and accumulating evidence suggests they affect your health differently.
This is what I want to walk you through today.

Oral micronized progesterone and the older synthetic progestins like medroxyprogesterone acetate (MPA) are not interchangeable molecules.
What Micronized Progesterone Actually Is — And Isn't
Your body has been making progesterone since puberty. It's produced mainly by the corpus luteum after ovulation, and later by the placenta during pregnancy. As you move through perimenopause and into postmenopause, production drops — sometimes steeply — and that hormonal shift contributes to symptoms that range from disruptive to genuinely distressing.
Micronized progesterone (brand name: Prometrium) is derived from plant sources, primarily wild yam, and the micronization process — breaking it into tiny particles — is what makes it absorbable when taken orally. It's FDA-approved, standardized, and regulated. When I prescribe it, I know exactly what my patients are getting.
This is different from compounded "bioidentical" progesterone preparations you'll find at some pharmacies. The word "bioidentical" gets used loosely in ways that can confuse patients. The research I'm sharing with you today is specifically about FDA-approved micronized progesterone — not compounded preparations, which lack standardized dosing and clinical outcome data. The Menopause Society is clear on this distinction [1].
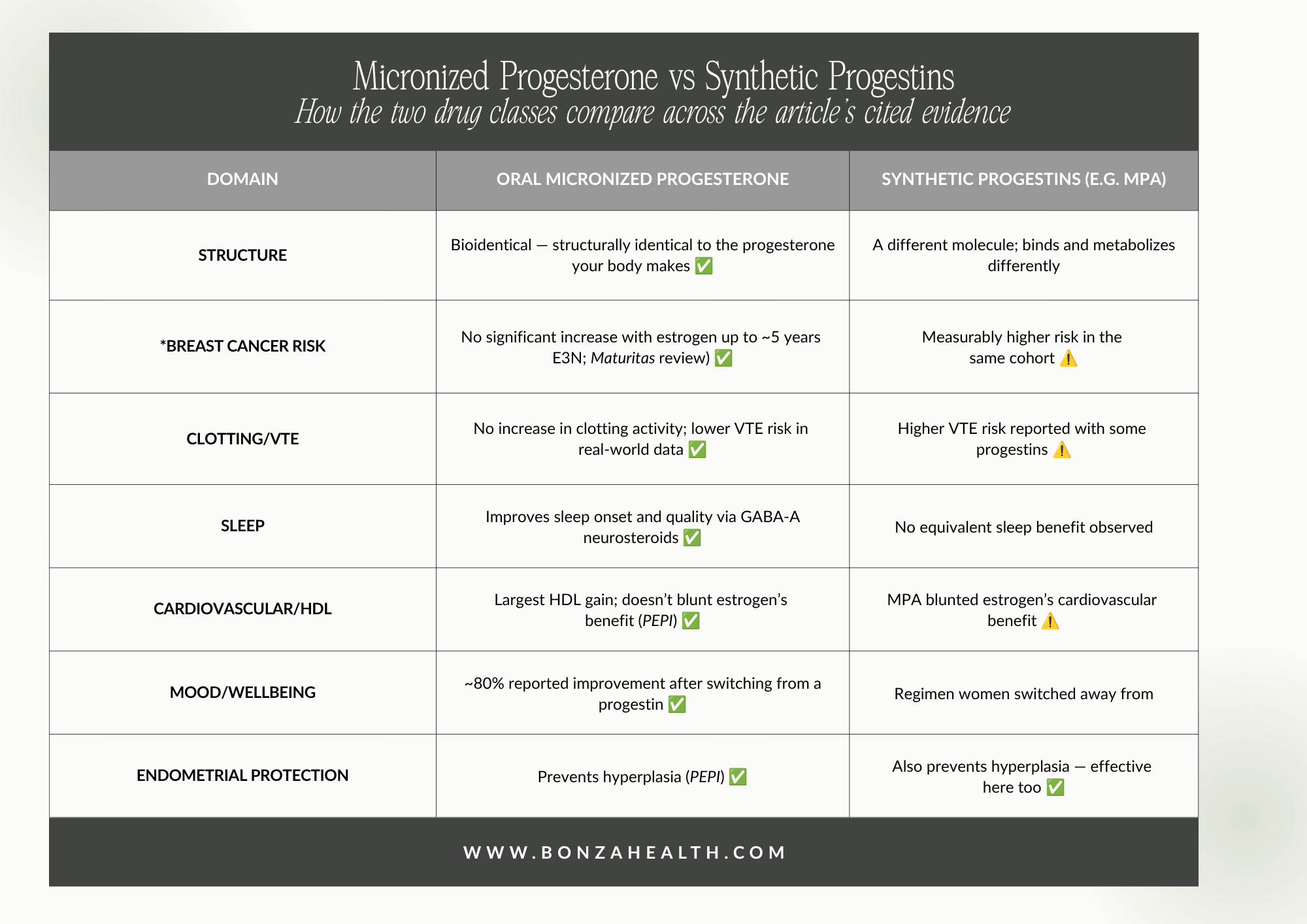
*Breast cancer data is strongest for use up to about five years; longer-term evidence is more limited.
This compares the two drug classes. It is not a statement that either is risk-free. Individual suitability depends on personal and family history.
Why I Take It Seriously for My Patients — And What the Evidence Shows
Sleep
This is where oral micronized progesterone has genuinely impressive data, and where the mechanism is worth understanding.
When your liver metabolizes micronized progesterone, it produces neuroactive steroids — allopregnanolone and pregnanolone — that act on GABA-A receptors in the brain. These are the same receptors targeted by benzodiazepines. The result is a natural calming effect on the nervous system. This is not sedation in a medicating-away-the-problem sense — it's your body's own inhibitory system being gently supported. It's why micronized progesterone is prescribed at bedtime, and why that timing isn't arbitrary.
A 2021 systematic review and meta-analysis in the Journal of Clinical Endocrinology & Metabolism analyzed nine randomized controlled trials and found that micronized progesterone improved sleep onset latency and overall sleep quality compared to placebo, with the majority of those trials enrolling postmenopausal women [2]. A head-to-head RCT comparing it directly to synthetic MPA found sleep efficiency improved by 8% in the micronized progesterone group, with no equivalent improvement in women taking the synthetic [3]. Sleep EEG studies confirmed reduced time awake and increased REM sleep in the first part of the night [4].
If you've told yourself that waking at 2 a.m. every night is just "part of menopause," I want you to know that it doesn't have to be.

Progesterone can have a natural calming effect on the nervous system.
Hot Flashes and Night Sweats
Micronized progesterone works for vasomotor symptoms — both in combination with estrogen and, for women who cannot or choose not to use estrogen, on its own. A randomized, placebo-controlled trial published in Menopause found women taking 300 mg nightly had meaningfully better vasomotor symptom scores than those on placebo [5]. A systematic review of progestin-only treatment found that a 300 mg dose was associated with nearly a 59% improvement in vasomotor symptoms, compared with approximately 24% in the placebo group [6].
That 59% figure is clinically significant. It means micronized progesterone is a legitimate option to discuss — particularly for women with contraindications to estrogen or those who prefer to start with progesterone alone.
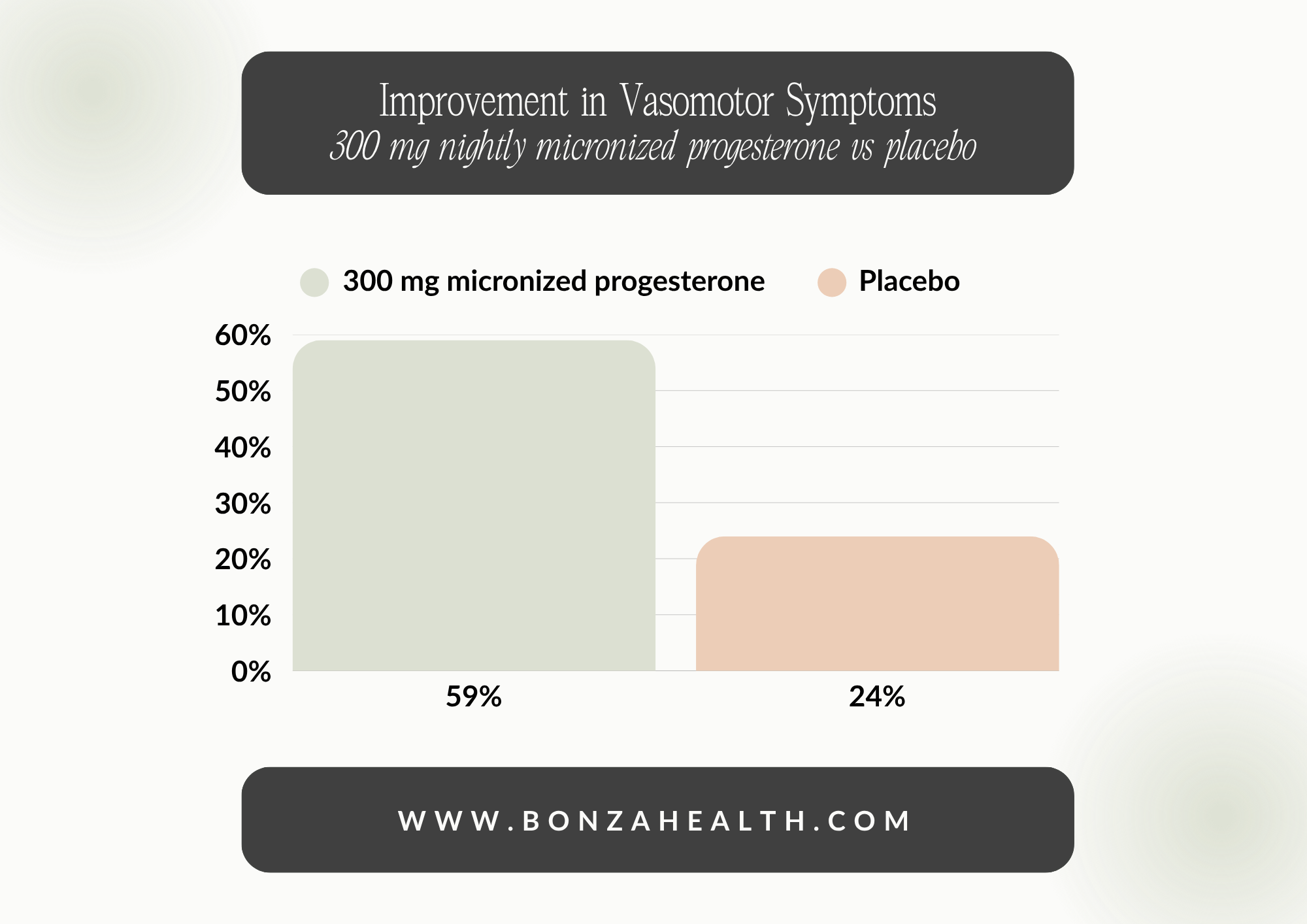
Source: Systematic review of progestin-only treatment. Both arms improve; the progesterone arm improves more than twice as much.
Breast Health
This is the question that weighs most heavily, and it deserves a direct answer rather than reassuring language that skirts around it.
The landmark E3N cohort study — a French prospective study following over 100,000 women — found that estrogen combined with micronized progesterone was not associated with a statistically significant increase in breast cancer risk, while estrogen combined with synthetic progestins carried a measurably higher risk [7]. This finding was replicated in updated E3N analyses and has since been supported by a systematic expert review published in Maturitas (2018), which concluded that estrogen with FDA-approved micronized progesterone does not increase breast cancer risk for up to five years of use [8].
The honest caveat: data beyond five years is more limited, and breast cancer risk should always be part of a personalized conversation with your physician — regardless of which hormone you use. But for many women, particularly those who stopped or avoided HRT because of the 2002 headlines, this data represents a meaningful reassessment.

Breast cancer risk should always be part of a personalized conversation with your physician
Endometrial Protection
If you have a uterus and you're taking systemic estrogen, progesterone is not optional — it's required to protect the uterine lining from the proliferative effects of estrogen. Unopposed estrogen causes endometrial hyperplasia and raises the risk of endometrial cancer.
The PEPI trial — a 3-year, randomized, double-blind, placebo-controlled study of 875 women — found that all progestogen-containing regimens, including those using micronized progesterone, prevented the hyperplasia that occurred in over 20% of women taking estrogen alone [9]. A multicenter study found that low daily doses of micronized progesterone effectively inhibited endometrial cell division and induced amenorrhea in over 90% of participants at three and six months [10,11].
One important nuance: consistent daily use matters for this protection. Because oral absorption can vary between individuals [12], taking it on the same schedule and communicating with your clinician about any unexpected bleeding is essential.

If you have a uterus and you're taking systemic estrogen, progesterone is not optional.
Cardiovascular and Lipid Effects
Heart disease is the leading cause of death in postmenopausal women. The cardiovascular profile of the progestogen you use matters.
The PEPI trial showed that among all active treatment regimens, the estrogen-plus-micronized-progesterone group had the highest HDL ("good" cholesterol) increase — and it did not blunt estrogen's cardiovascular benefit the way synthetic MPA did [9]. Research also indicates that micronized progesterone does not increase clotting factor activity or venous thromboembolism (VTE) risk, a meaningful difference from some synthetic progestins [13,14]. A 2023 real-world evidence study found that oral estradiol combined with micronized progesterone was associated with significantly lower VTE risk compared to oral conjugated estrogens combined with MPA [15].

The cardiovascular profile of the progestogen you use matters.
Mood, Calm, and Brain Health
Those calming neurosteroids described in the sleep section do more than help you sleep. In surveys of women who switched from synthetic progestins to micronized progesterone, the majority reported improvements in mood, anxiety, and overall wellbeing — with around 80% expressing satisfaction with the change [16].
On neuroprotection, the science is genuinely promising but still evolving. Preclinical and animal models show robust neuroprotective effects from progesterone — effects that synthetic progestins appear not to share [17], [18]. Human studies on memory and cognition have been more mixed, and I won't overstate what we know. What I do tell my patients is that there is a proposed "critical window" early in the menopause transition when hormonal support for the brain may matter most — which is one more reason that early, individualized care matters.

There is a proposed "critical window" early in the menopause transition when hormonal support for the brain may matter most — which is one more reason that early, individualized care matters.
Bone Density
Bone loss accelerates sharply in the first decade after menopause. The PEPI trial confirmed that hormone therapy regimens including micronized progesterone improved bone mineral density compared to placebo [9]. A 2013 randomized trial from Mayo Clinic found that estrogen with micronized progesterone prevented deterioration of cortical bone and cortical porosity — changes that occurred in the placebo group over the same period [19].

Bone loss accelerates sharply in the first decade after menopause.
What I Tell My Own Patients
The 2022 Menopause Society position statement — endorsed by more than 20 international organizations [1] — affirmed something I have believed throughout my clinical career: hormone therapy risk and benefit depend significantly on which hormone you use, not just whether you use it. The era of treating all progestogens as equivalent is over.
That does not mean micronized progesterone is right for every woman. It is not. Hormone therapy requires a real evaluation of your personal health history, your symptoms, your priorities, and your risk factors. But it does mean that the category of "I'm afraid of hormones" deserves to be reopened and examined with current evidence — not settled by a headline.
At Bonza Health, I built a practice around exactly that kind of conversation. Women tell me what they're experiencing. We look at what the evidence says. We build a plan together.
If you've been tolerating sleep disruption, mood changes, hot flashes, or fatigue because you thought your options were limited — they aren't.

Hormone therapy requires a real evaluation of your personal health history, your symptoms, your priorities, and your risk factors.
A Few Things Worth Knowing Before You Start Any Conversation With a Clinician
Micronized progesterone is sedating, which is why it's taken at bedtime. Daytime use can cause significant grogginess.
Absorption varies between individuals. If you're taking it for endometrial protection, consistency of use is not negotiable.
FDA-approved Prometrium and compounded progesterone are not the same product. If a compounding pharmacy is framing its preparation as equivalent, ask for outcome data — because it doesn't exist.
If you've had breast cancer, thromboembolism, unexplained vaginal bleeding, or certain liver conditions, progesterone therapy requires a detailed conversation with a specialist before proceeding.
The goal of sharing this isn't to convince you that micronized progesterone is the answer. It's to make sure that when you sit down with a clinician — whether that's me or someone else — you're asking the right questions.
Ready to have that conversation?

Bonza Health is a telemedicine practice built for women in perimenopause and postmenopause — women who are done being brushed off and ready for personalized, evidence-based care. Schedule a virtual visit and let's look at the full picture together.
This article reflects current peer-reviewed research and the 2022 clinical guidelines from The Menopause Society. It is written for educational purposes and does not constitute individualized medical advice. Hormone therapy is not appropriate for everyone. Please speak with a qualified clinician about your complete personal and family history before starting or modifying any treatment.
References
[1] The Menopause Society Advisory Panel, "The 2022 hormone therapy position statement of The North American Menopause Society," Menopause, vol. 29, no. 7, pp. 767–794, Jul. 2022, https://doi.org/10.1097/gme.0000000000002028
[2] K. E. Ensrud, H. Joffe, K. A. Guthrie, et al., "Efficacy of micronized progesterone for sleep: a systematic review and meta-analysis of randomized controlled trial data," J. Clin. Endocrinol. Metab., vol. 106, no. 4, pp. 942–951, Apr. 2021, https://doi.org/10.1210/clinem/dgaa873
[3] J. Montplaisir, J. Lorrain, R. Denesle, and D. Petit, "Sleep in menopause: differential effects of two forms of hormone replacement therapy," Menopause, vol. 8, no. 1, pp. 10–16, 2001. https://doi.org/10.1097/00042192-200101000-00004
[4] P. Schüssler, M. Kluge, A. Yassouridis, et al., "Progesterone reduces wakefulness in sleep EEG and has no effect on cognition in healthy postmenopausal women," Psychoneuroendocrinology, vol. 33, no. 8, pp. 1124–1131, 2008, https://doi.org/10.1016/j.psyneuen.2008.05.013
[5] C. L. Hitchcock and J. C. Prior, "Oral micronized progesterone for vasomotor symptoms—a placebo-controlled randomized trial in healthy postmenopausal women," Menopause, vol. 19, no. 8, pp. 886–893, 2012, https://doi.org/10.1097/gme.0b013e318247f07a
[6] C. A. Stuenkel, S. R. Davis, A. Gompel, et al., "Efficacy of progestin-only treatment for the management of menopausal vasomotor symptoms," Johns Hopkins University, 2021. [Online]. Available: https://pure.johnshopkins.edu/en/publications/efficacy-of-progestin-only-treatment-for-the-management-of-menopa
[7] A. Fournier, F. Berrino, and F. Clavel-Chapelon, "Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study," Breast Cancer Res. Treat., vol. 107, no. 1, pp. 103–111, 2008, https://doi.org/10.1007/s10549-007-9523-x
[8] N. Asi, K. Mohammed, Q. Haydour, et al., "The impact of micronized progesterone on breast cancer risk: a systematic review," Maturitas, vol. 88, pp. 57–64, 2016 (updated 2018), https://doi.org/10.1080/13697137.2017.1421925
[9] Writing Group for the PEPI Trial, "Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in postmenopausal women: the Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial," JAMA, vol. 273, no. 3, pp. 199–208, 1995, https://doi.org/10.1001/jama.1995.03520270033028.
[10] D. L. Moyer, B. de Lignieres, P. Driguez, and J. P. Pez, "Prevention of endometrial hyperplasia by progesterone during long-term estradiol replacement: influence of bleeding pattern and secretory changes," Fertil. Steril., vol. 59, no. 5, pp. 992–997, 1993. https://doi.org/10.1016/s0015-0282(16)55916-0
[11] A. L. Murkes, P. Conner, K. Leifland, and E. Lundstrom, "Progesterone and endometrial cancer," Best Pract. Res. Clin. Obstet. Gynaecol., vol. 69, pp. 1–13, 2020, https://doi.org/10.1016/j.bpobgyn.2020.05.003
[12] R. A. Miles, R. J. Paulson, R. A. Lobo, M. F. Press, L. Dahmoush, and M. V. Sauer, "Pharmacokinetics and endometrial tissue levels of progesterone after administration by intramuscular and vaginal routes: a comparative study," Pharmacotherapy, vol. 14, no. 6, pp. 695–699, 1994. https://doi.org/10.1016/s0015-0282(16)56935-0
[13] T. Römer, J. Bitzer, and D. Foth, "The impact of micronized progesterone on cardiovascular events," Maturitas, vol. 162, pp. 65–72, 2022, https://doi.org/10.1080/13697137.2021.2022644
[14] M. Canonico, E. Oger, and P. Y. Scarabin, "Progestogens and venous thromboembolism among postmenopausal women using hormone therapy," Maturitas, vol. 70, no. 4, pp. 354–360, 2011, https://doi.org/10.1016/j.maturitas.2011.10.002
[15] A. Ní Fhaoláin, C. Mullaney, and B. Healy, "Oral estradiol/micronized progesterone may be associated with lower venous thromboembolism risk than oral CEE/MPA," Maturitas, 2023, https://doi.org/10.1016/j.maturitas.2023.04.004
[16] L. A. Fitzpatrick, C. Pace, and B. Wiita, "Comparison of regimens containing oral micronized progesterone or medroxyprogesterone acetate on quality of life in postmenopausal women: a cross-sectional survey," J. Womens Health Gend. Based Med., vol. 9, no. 4, pp. 381–387, 2000, https://doi.org/10.1089/15246090050020691
[17] R. D. Brinton, J. K. Liu, J. Yao, and L. Zhao, "Progesterone-induced neuroprotection: factors that may predict therapeutic efficacy," Brain Res., vol. 1514, pp. 98–106, 2013, https://doi.org/10.1016/j.brainres.2013.01.027
[18] J. Nilsen and R. D. Brinton, "Mechanisms of progesterone-induced neuroprotection," Ann. N. Y. Acad. Sci., vol. 1052, pp. 145–151, 2005, https://doi.org/10.1196/annals.1347.010
[19] J. N. Farr, S. Khosla, S. J. Achenbach, et al., "Effects of estrogen with micronized progesterone on cortical and trabecular bone mass and microstructure in recently postmenopausal women," J. Clin. Endocrinol. Metab., vol. 98, no. 2, pp. E249–E257, 2013, https://doi.org/10.1210/jc.2012-3406