
The Truth About Perimenopause and Your Mood
Written and edited by Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Why anxiety and depression in your early 40s may not be “just stress” — and why your doctor might be missing the real cause.
Last week, a patient sat in my office and told me a story I have heard far too many times. She was 42 years old. Over the past year, she had developed new-onset anxiety and depression that felt unlike anything she had experienced before. She went to four different doctors. Each one had a different recommendation. One said it was stress. Another prescribed an antidepressant. A third suggested therapy. Her gynecologist told her she was “too young” for hormonal changes and dismissed her concerns entirely.
She asked every single one of them about her hormones. Not one took her seriously.
Her story is not unique. It is the story of millions of women whose early perimenopausal hormonal shifts are dismissed, overlooked, or misattributed to life circumstances. And it is a story we need to change.
Perimenopause Begins Earlier Than You Think
Most women associate hormonal changes with menopause itself, which is defined as one full year after your last menstrual period and occurs at an average age of 51 [1]. But perimenopause — the transitional phase leading up to menopause — typically begins between ages 42 and 52 [2]. For some women, subtle hormonal fluctuations start even in their late 30s.
During early perimenopause, estrogen does not simply decline in a straight line. Instead, it fluctuates wildly and unpredictably. Some months estrogen surges higher than normal; other months it drops dramatically. It is this variability — not just the eventual decline — that wreaks havoc on a woman’s brain chemistry, mood, and emotional resilience [3,4].

The Study of Women’s Health Across the Nation (SWAN), one of the largest longitudinal studies on women and midlife health, clearly demonstrated that mood changes — including depressive symptoms and anxiety — are associated with the perimenopausal transition [5]. The Harvard Study of Moods and Cycles confirmed that women entering perimenopause had a significantly increased risk of first-onset depression, even among those with no prior history of mood disorders [6]. Depressive symptoms experienced in perimenopause are often more severe than those seen before or after the transition [2].
Estrogen Is Not Just a Reproductive Hormone: It’s a Brain Hormone
Estradiol, the most potent form of estrogen, is one of the most powerful regulators of brain chemistry we have. Estradiol receptors are distributed widely throughout the brain, where they influence memory, neuroprotection, neurogenesis, cerebral blood flow, and — critically — the synthesis and turnover of key neurotransmitters including serotonin and dopamine [7,8].
When estrogen levels are stable, these neurotransmitter systems function smoothly. When estrogen fluctuates erratically, as it does in perimenopause, the downstream effects on serotonin and dopamine can be profound.
Serotonin and Dopamine: What They Do and What Happens When They Decline
Serotonin is often called the “feel-good” neurotransmitter. It regulates mood stability, sleep, appetite, digestion, and emotional resilience. When serotonin levels are disrupted, women may experience persistent sadness, increased anxiety, difficulty sleeping, irritability, carbohydrate cravings, reduced motivation, and a sense that their emotional “buffer” has disappeared [9].
Dopamine is the brain’s reward and motivation chemical. It drives feelings of pleasure, focus, ambition, and satisfaction. When dopamine declines, women often describe feeling flat, unmotivated, unable to experience joy from things they once loved (anhedonia), experiencing brain fog, and a loss of drive [10].
Estrogen directly modulates the production and receptor sensitivity of both neurotransmitters. The erratic hormonal swings of perimenopause disrupt these systems, producing mood symptoms that can range from subtle unease to debilitating depression and anxiety [8,11].
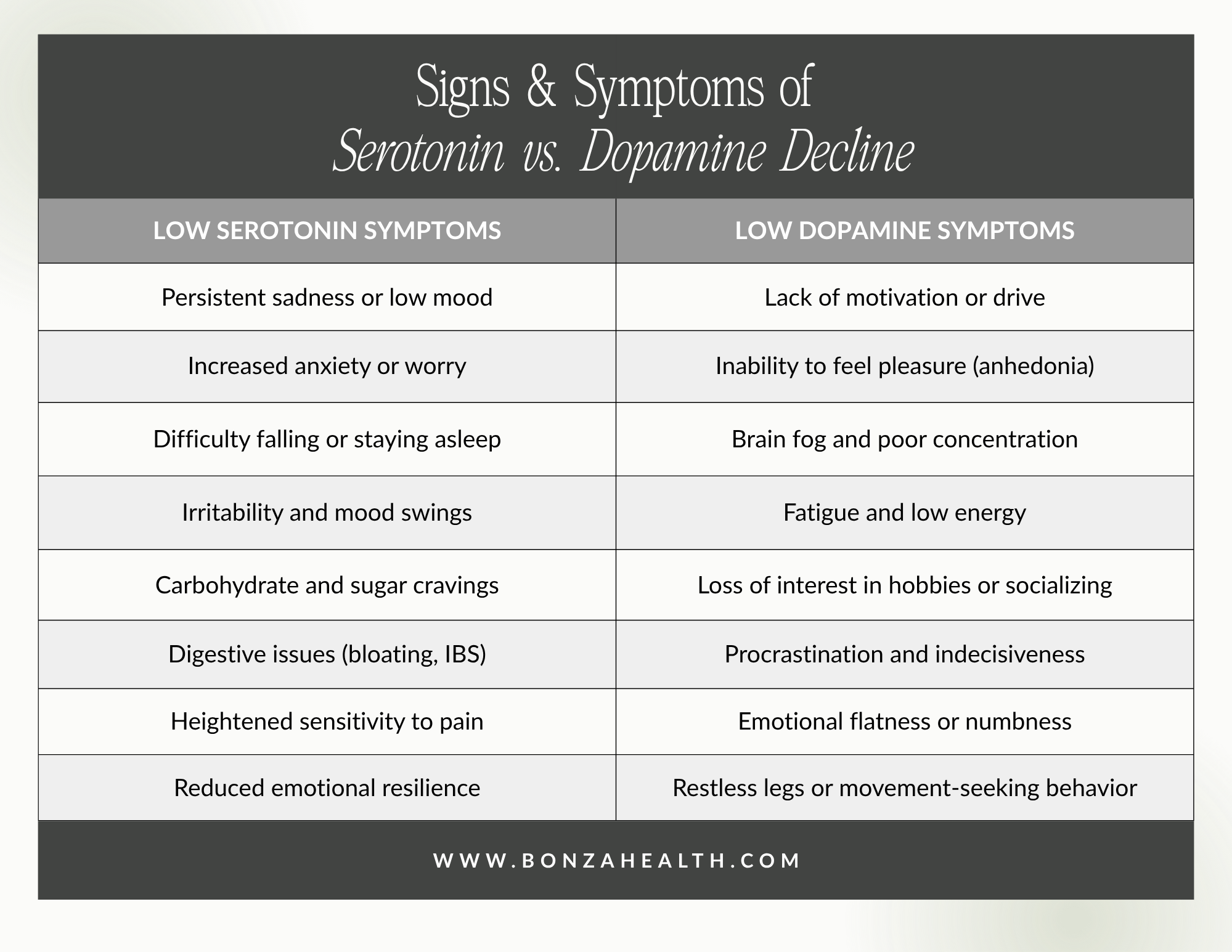
Signs and symptoms of serotonin vs. dopamine decline
The Estrogen–Gut–Mood Connection: The Estrobolome
Here is a piece of the puzzle that most doctors are not discussing: approximately 90% of the body’s serotonin and approximately 50% of its dopamine are produced not in the brain, but in the gut [12,13]. Gut bacteria play a direct role in stimulating the intestinal cells that synthesize these neurotransmitters.
A specialized collection of microbes in the gut, known as the estrobolome, is responsible for metabolizing estrogen. These bacteria produce enzymes, primarily beta-glucuronidase, that reactivate estrogen and regulate how much circulating estrogen is available in your body [14,15]. When the gut microbiome is healthy and diverse, the estrobolome functions well, supporting stable estrogen levels. When gut health is compromised — through stress, poor diet, antibiotic use, or aging — the estrobolome becomes dysregulated, further depleting circulating estrogen and compounding the neurotransmitter disruption already occurring during perimenopause [14].
This creates a vicious cycle: declining estrogen reduces gut microbial diversity, which further impairs estrogen metabolism, which further reduces serotonin and dopamine production.
Why Mood Trouble Gets Worse During Perimenopause
The combination of erratic estradiol fluctuations, disrupted neurotransmitter synthesis, estrobolome dysfunction, and the downstream effects on sleep, cognition, and stress resilience means that mood symptoms tend to intensify as perimenopause progresses. The SWAN study found that the risk of high depressive symptoms increased with the start of the menopausal transition and remained elevated through early postmenopause [5]. Women under high life stress during this period are particularly vulnerable [3,4].
This is not “just stress.” This is neurochemistry. And it deserves to be treated as such.
Perimenopause can wreak havoc on a woman’s brain chemistry and mood
Treatment: Why You Should Not Wait Until Menopause
One of the most damaging misconceptions in women’s health is the idea that hormone therapy should only be considered after menopause is confirmed. The research tells a very different story.
A landmark 2018 randomized clinical trial by Gordon et al., published in JAMA Psychiatry, demonstrated that 12 months of transdermal estradiol combined with intermittent micronized progesterone was significantly more effective than placebo in preventing the development of clinically significant depressive symptoms among perimenopausal and early postmenopausal women. In the placebo group, 32.3% developed clinically significant depression, compared to only 17.3% in the treatment group [4]. The benefit was especially pronounced in women experiencing high life stress.
Transdermal estradiol (delivered through a patch or gel) is the preferred delivery method because it closely mimics the body’s natural estrogen, effectively crosses the blood-brain barrier, and avoids first-pass liver metabolism [16]. Micronized progesterone (such as Prometrium) is the bioidentical form of progesterone and, unlike synthetic progestins, does not counteract the mood benefits of estrogen and may itself have calming, sleep-promoting properties [17].
The North American Menopause Society consensus statement supports the use of hormone therapy in symptomatic perimenopausal women when benefits outweigh risks [16]. You do not need to wait until you have gone 12 months without a period to seek help.
The Bottom Line
Perimenopause is not something to simply endure. The mood changes you are experiencing are not a personal failing, not “just stress,” and not something you should accept as normal aging. They are the result of real neurochemical changes driven by hormonal fluctuations — and they are treatable.
If you are a woman in your late 30s, 40s, or early 50s experiencing new or worsening anxiety, depression, brain fog, or emotional flatness, advocate for yourself. Ask your provider about your hormones. You deserve to feel like yourself again.
In Blog 2, we dive deeper into how you can support your serotonin and dopamine production naturally with evidence-based supplements — and take a closer look at the estrobolome.

Schedule your evaluation with Dr. Bonza to receive 12 months of menopause care
References:
[1] S. Alblooshi, M. Taylor, and N. Gill, “Does menopause elevate the risk for developing depression and anxiety? Results from a systematic review,” Australas. Psychiatry, vol. 31, no. 2, pp. 165–173, 2023. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC10088347/
[2] M. Herson and J. Kulkarni, “Hormonal agents for the treatment of depression associated with the menopause,” Drugs Aging, vol. 39, pp. 607–618, 2022. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC9355926/
[3] J. L. Gordon, D. R. Rubinow, T. A. Eisenlohr-Moul, J. Leserman, and S. S. Girdler, “Estradiol variability, stressful life events, and the emergence of depressive symptomatology during the menopausal transition,” Menopause, vol. 23, no. 3, pp. 257–266, 2016.
[4] J. L. Gordon, D. R. Rubinow, T. A. Eisenlohr-Moul, K. Xia, P. J. Schmidt, and S. S. Girdler, “Efficacy of transdermal estradiol and micronized progesterone in the prevention of depressive symptoms in the menopause transition: A randomized clinical trial,” JAMA Psychiatry, vol. 75, no. 2, pp. 149–157, 2018. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC5838629/
[5] J. T. Bromberger et al., “Depressive symptoms during the menopausal transition: The Study of Women’s Health Across the Nation (SWAN),” J. Affect. Disord., vol. 103, pp. 267–272, 2007. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC2048765/
[6] L. S. Cohen, C. N. Soares, A. F. Vitonis, M. W. Otto, and B. L. Harlow, “Risk for new onset of depression during the menopausal transition: The Harvard Study of Moods and Cycles,” Arch. Gen. Psychiatry, vol. 63, no. 4, pp. 385–390, 2006.
[7] Editorial, “Hormone replacement therapy for menopausal mood swings and sleep quality: The current evidence,” World J. Psychiatry, 2024. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC11514567/
[8] N. Deshpande and T. S. Sathyanarayana Rao, “Psychological changes at menopause: Anxiety, mood swings, and sexual health in the biopsychosocial context,” Indian J. Psychiatry, 2025. doi: 10.1177/26318318251324577.
[9] T. A. Jenkins, J. C. D. Nguyen, K. E. Polglaze, and P. P. Bertrand, “Influence of tryptophan and serotonin on mood and cognition with a possible role of the gut-brain axis,” Nutrients, vol. 8, no. 1, p. 56, 2016.
[10] N. Musial, Z. Ali, J. Grbevski, A. Veerakumar, and P. Sharma, “Perimenopause and first-onset mood disorders: A closer look,” Focus (Am. Psychiatr. Publ.), vol. 19, no. 3, pp. 330–337, 2021. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC8475932/
[11] K. M. Albert, P. A. Newhouse, “Estrogen, stress, and depression: Cognitive and biological interactions,” Annu. Rev. Clin. Psychol., 2019. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC9673602/
[12] M. Y. Lam et al., “Gut microbiota as an endocrine organ: Unveiling its role in human physiology and health,” Appl. Sci., vol. 14, no. 20, art. no. 9383, 2024. doi: 10.3390/app142093830.
[13] O. G. Ogunrinola et al., “Impact of probiotics and prebiotics on gut microbiome and hormonal regulation,” Challenges, vol. 6, no. 4, art. no. 56, 2024. doi: 10.3390/challe6040056.
[14] J. M. Baker, L. Al-Nakkash, and M. M. Herbst-Kralovetz, “Estrogen–gut microbiome axis: Physiological and clinical implications,” Maturitas, vol. 103, pp. 45–53, 2017. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/28778332/
[15] R. K. Kaliannan et al., “From gut to hormones: Unraveling the role of gut microbiota in (phyto)estrogen modulation in health and disease,” Mol. Nutr. Food Res., 2024. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/38342595/
[16] C. N. Soares, “Optimal management of perimenopausal depression,” Int. J. Women’s Health, vol. 2, pp. 143–151, 2010. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC2971729/
[17] X. Zhang et al., “Role of estrogen in treatment of female depression,” Front. Pharmacol., 2024. [Online]. Available: https://pmc.ncbi.nlm.nih.gov/articles/PMC10911346/