
Subcutaneous vs. Sublingual GLP-1s in Perimenopause: A Cautious Physician's Honest Look at the Evidence
Written and edited by Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Why the route of GLP-1 administration matters — and where the marketing has run ahead of the published data.
A patient brought a pamphlet to her appointment last month. It was from a telehealth platform she had been considering. The pamphlet promised "GLP-1 sublingual drops — no injections, no commitment, no side effects." It was $189 a month. She wanted to know what I thought.
I think about that pamphlet a lot. I think about how compelling the language was — how it spoke directly to every concern a 48-year-old woman in perimenopause might have about starting a GLP-1: the needles, the gastrointestinal side effects, the social weight of "being on Ozempic," the price tag of brand-name medications. I think about how the published clinical evidence underneath those promises is much thinner than the pamphlet suggests. And I think about how the woman across from me deserved an honest answer, not a sales pitch in either direction.
I should be transparent before going further. I have personal experience with this class of medication. After gaining weight during the pandemic — like so many of my patients — I tried subcutaneous semaglutide myself. I experienced severe nausea and vomiting for weeks and was not able to continue. That experience shapes how I think about prescribing GLP-1 medications today. I respect what these drugs can do clinically. I am also clear-eyed about who they are not the right fit for, and I do not prescribe them with the enthusiasm I see in some corners of the wellness-medicine marketplace.
What follows is what I think about subcutaneous versus sublingual GLP-1s in perimenopause, where the evidence is strong, where it is thin, and how a physician committed to both honesty and accessibility thinks through this.

Weight gain is a common complaint during perimenopause. For some women, GLP-1 medications may help with weight management.
Why GLP-1 medications matter in perimenopause
Estrogen decline in perimenopause and menopause drives measurable changes in body composition, insulin sensitivity, and visceral fat accumulation. Many of my patients describe gaining weight in their forties despite eating and exercising the same way they always have. They are not imagining this. The hormonal context has changed, and the metabolic machinery that used to work no longer works the same way.
GLP-1 receptor agonists — semaglutide (Ozempic, Wegovy), tirzepatide (Mounjaro, Zepbound, which is technically a dual GLP-1/GIP agonist), and liraglutide (Saxenda, Victoza) — act through a combination of slowed gastric emptying, central appetite regulation, glucose-dependent insulin secretion, and improvements in insulin sensitivity [1,2]. In randomized controlled trials, weekly subcutaneous semaglutide produced approximately 15% body weight loss at 68 weeks in adults with obesity [1]. Tirzepatide produced approximately 20% body weight loss at 72 weeks [2]. The SELECT trial extended these findings to cardiovascular outcomes, showing semaglutide reduced major adverse cardiovascular events in adults with overweight or obesity and pre-existing cardiovascular disease [3].
These are some of the most robust outcome data we have for any chronic-disease medication. The benefits are real. The side effects are also real, and they are not minor for a substantial subset of patients. Both of these facts deserve equal weight in the conversation about which form to use.
At a glance: how the three routes compare
Before walking through each form in detail, here is the landscape in a single view.
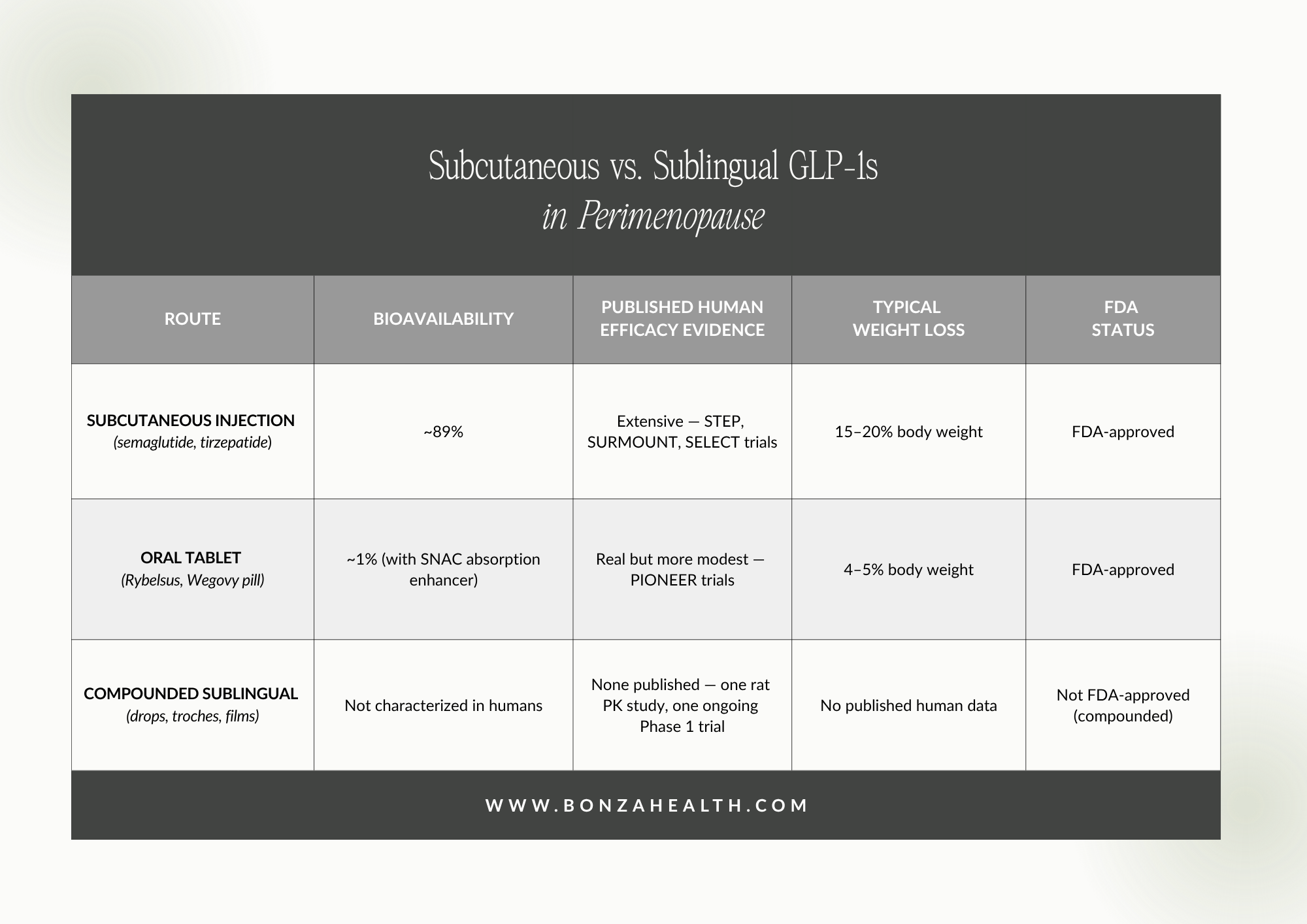
Subcutaneous vs. sublingual GLP-1s in perimenopause.
The rest of this article walks through what each row in that table actually means, and how I think about it clinically.
Subcutaneous injection: where the evidence is built
This is the form that built the entire clinical case for GLP-1s. Subcutaneous semaglutide has an absolute bioavailability of approximately 89%, achieves peak plasma concentration within 1 to 3 days, and reaches steady state after roughly 4 to 5 weeks of weekly administration [4]. The elimination half-life is approximately one week, which is what makes once-weekly dosing pharmacologically rational rather than a marketing convenience.
Every major efficacy trial of semaglutide and tirzepatide for weight management, glycemic control, and cardiovascular outcomes was conducted with the subcutaneous formulation [1-3]. When we talk about "GLP-1s work for weight loss," we are almost always talking about subcutaneous GLP-1s. This is the form with the strongest evidence and the form I would consider first for patients who are appropriate candidates and able to tolerate the medication.
The "able to tolerate" qualifier is doing real work in that sentence. Gastrointestinal side effects — nausea, vomiting, delayed gastric emptying, sometimes severe — are common, often dose-dependent, and not always manageable through standard titration. Some patients experience meaningful side effects even at the lowest doses. I am one of those patients. I share this with women in my practice because they deserve to know that the side effect profile is not a footnote.

Estrogen decline in perimenopause and menopause drives measurable changes in body composition, insulin sensitivity, and visceral fat accumulation.
Oral tablet: FDA-approved, with trade-offs
In 2019, the FDA approved Rybelsus, an oral tablet form of semaglutide for type 2 diabetes. Rybelsus pairs semaglutide with an absorption enhancer called SNAC (sodium N-(8-(2-hydroxybenzoyl) amino) caprylate), which temporarily creates a localized environment in the stomach that allows the peptide to be absorbed before being degraded by digestive enzymes.
The PIONEER trials demonstrated that oral semaglutide is more effective than placebo and comparable to other diabetes medications for glycemic control [5]. PIONEER 4 found oral semaglutide non-inferior to subcutaneous liraglutide for HbA1c reduction over 26 weeks [6].
Two limitations matter clinically. First, the bioavailability of oral semaglutide is approximately 1% — meaning that of the dose swallowed, only about one percent reaches the bloodstream in active form, even with the SNAC absorption enhancer [5,6]. Second, absorption is highly sensitive to timing and gastric conditions: Rybelsus must be taken on an empty stomach, with no more than 4 ounces of plain water, followed by a 30-minute fast. Food, beverages, or other medications during that window dramatically reduce absorption. The result is that oral semaglutide typically produces 4 to 5% weight loss versus 15 to 17% with injectable semaglutide [5,7]. It is a useful option for patients who genuinely cannot or will not use injections, but the trade-off should be understood.
In January 2026, the FDA approved a higher-dose oral semaglutide formulation marketed as the Wegovy pill specifically for weight management, expanding the FDA-approved oral options for women who want a pill rather than an injection.

In 2019, the FDA approved Rybelsus, an oral tablet form of semaglutide for type 2 diabetes. It may also be used for menopause-related weight management in some situations.
Compounded sublingual: where the marketing runs ahead of the evidence
This is where I want to be most honest, because this is where the gap between marketing and published evidence is widest, and where my own caution is strongest.
Compounded sublingual semaglutide and tirzepatide have proliferated through telehealth platforms over the past several years. The theoretical rationale is reasonable: peptides taken orally are degraded by stomach acid and digestive enzymes, so bypassing the digestive tract by absorbing through the sublingual mucosa might preserve more of the active drug. The marketing language frequently includes claims of "optimal bioavailability" and "comparable efficacy" to injections.
Here is the problem. As of this writing, there are no published peer-reviewed human clinical trials demonstrating efficacy of sublingual semaglutide or tirzepatide for weight loss, glycemic control, or any clinical endpoint. The published evidence consists almost entirely of:
Preclinical animal data, including a 2025 rat pharmacokinetic study demonstrating that sublingual semaglutide is detectable in rat plasma within minutes of administration [8]. The authors of that study explicitly note that rat pharmacokinetics differ substantially from human pharmacokinetics — rat albumin turnover is 2 days versus 25 days in humans — and they describe their work as proof-of-concept, not clinical evidence.
An ongoing Phase 1 clinical trial of sublingual liraglutide in patients with type 2 diabetes (NCT05268237), which has not yet reported results.
Manufacturer and compounding-pharmacy promotional materials that often cite the rat data or the theoretical mechanism without acknowledging the absence of published human efficacy data.
When a telehealth platform tells a patient that sublingual GLP-1 drops will provide "the same results as injections," that claim is currently not supported by published clinical trial evidence in humans. The biological plausibility is real. The clinical proof is not. That is not a small distinction in medicine.

Currently, there are no published peer-reviewed human clinical trials demonstrating efficacy of sublingual semaglutide or tirzepatide for weight loss, glycemic control, or any clinical endpoint.
How I think about prescribing this class of medication
Given the evidence picture and my own experience, here is the framework I actually use.
For patients who are appropriate candidates and can tolerate the medication, FDA-approved subcutaneous semaglutide or tirzepatide is my preferred form. The evidence is the strongest, the dosing is the most well-characterized, and the regulatory framework provides the most patient protection.
For patients who cannot tolerate injections, who have specific reasons that injection is not viable, or whose access to FDA-approved formulations is limited despite recent manufacturer price reductions, I am willing to consider FDA-approved oral semaglutide. The evidence for it is less impressive than for injections but it exists, and it is regulated.
For sublingual compounded formulations, my position is one of significant caution. The published human evidence is essentially absent. The marketing claims often outrun what can be defended in the literature. When I do consider these formulations — and I want to be honest that I do, in narrow circumstances, for patients who cannot access FDA-approved options — I do so with explicit informed consent. That conversation includes the absence of published human efficacy data, the limited regulatory oversight of the specific formulation, the potential for inconsistency between products, and the clear preference for FDA-approved alternatives whenever those are accessible. This is a conversation, not a checkbox. Patients deserve to know what they are taking and what they are not.
Who should not use GLP-1 medications
Regardless of route, GLP-1 receptor agonists are not appropriate for every patient. The following are situations that change the conversation significantly and warrant either avoidance or specialist co-management.
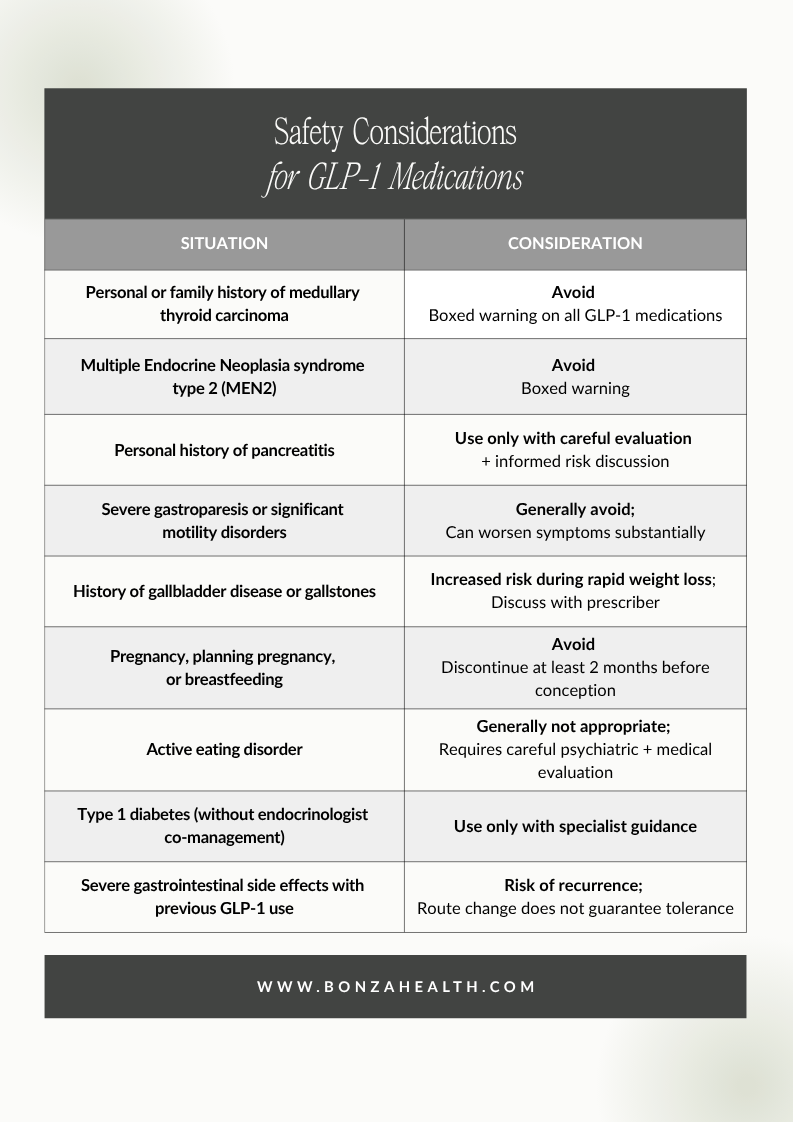
Safety considerations for GLP-1 medications.
The most common side effects across all routes — nausea, vomiting, diarrhea, constipation, delayed gastric emptying — are well documented and often improve with slower titration. They are not minor for everyone, which is part of why thoughtful candidate selection matters more than enthusiasm.
A note on access
I want to acknowledge the financial reality that drives many of these conversations. Brand-name injectable GLP-1s, even with manufacturer direct-to-consumer programs, frequently cost between $600 and $1,400 per month out of pocket once a patient is at maintenance dosing or buying through standard retail pharmacy channels. That is $7,000 to $17,000 per year. Many women cannot reasonably afford that. Insurance coverage for weight-management indications remains inconsistent, often requires prior authorization with extensive documentation, and frequently excludes the indication entirely — meaning even patients with insurance often pay near-retail prices.
This is not a failure of patients. It is a failure of the system. And it is part of why compounded formulations have grown so dramatically in the marketplace. Affordability is a legitimate clinical concern, and any honest discussion of GLP-1 therapy has to acknowledge it.
What GLP-1 medications actually cost
The pricing landscape is complicated, and the number a patient actually pays depends on the dose, the pharmacy, whether insurance covers the weight-management indication, and whether the patient qualifies for manufacturer direct-to-consumer programs. The ranges below reflect what patients are realistically paying in 2026, not the best-case advertised price.

What GLP-1 medications actually cost.
A few realities worth naming. Manufacturer direct-to-consumer pricing is real but generally applies to specific doses, requires self-pay status (no government insurance), and may not be available at maintenance doses where most patients eventually land. Insurance coverage for weight-management indications remains inconsistent — even patients with insurance frequently face $600 to $1,200 monthly out-of-pocket costs after rejected prior authorizations or formulary exclusions. And compounded pricing varies significantly between telehealth platforms.
What I can do as a physician is help patients understand what their real options are, not the headline-rate version. The FDA-approved Wegovy pill, launched in early 2026, has expanded the oral options at meaningfully lower price points than injectables for many patients. For some, that is the answer. For others, compounded options are the practical reality, and the conversation becomes one of informed risk rather than ideal evidence.
I would rather have an honest conversation with a patient about her real options than have her purchase something through a marketing channel that does not give her the full picture.

Insurance coverage for weight-management indications remains inconsistent — even patients with insurance frequently face $600 to $1,200 monthly out-of-pocket costs after rejected prior authorizations or formulary exclusions.
My honest take
GLP-1 medications are some of the most clinically important agents introduced in our lifetime for metabolic health. They are also some of the most over-promised. The subcutaneous evidence is excellent. The FDA-approved oral evidence is real but more modest. The sublingual evidence in humans does not yet exist in any meaningful way.
If you are a perimenopausal woman considering GLP-1 therapy, please do not let the convenience of a sublingual drop or the price difference between compounded and brand-name be the basis of your decision in isolation. Ask the platform you are considering: where is the published human efficacy data for this specific formulation? Who is monitoring me? What happens if I have side effects?
This is the conversation I am here to have with you. Carefully. Honestly. With respect for what these medications can do and equal respect for who they are not the right answer for. That includes, sometimes, the doctor writing this article.
Ready to figure out whether GLP-1 therapy — or another approach — is the right tool for you?
If this article describes where you are, I would love to help you think it through.
→ Take the Bonza Health hormone quiz to see if a consultation is a good fit.
→ Book a 50-minute consultation with Dr. Bonza — we'll look at your full picture, discuss whether GLP-1 therapy is appropriate, which form makes sense for you, and how it fits into the larger plan for your perimenopausal health.
Related reading on Bonza Health:

Dr. Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC is a board-certified Family Physician and Certified Menopause Practitioner serving women in Ohio and beyond. Bonza Health is licensed to practice in Ohio. GLP-1 medications, when prescribed, are managed with appropriate evaluation, monitoring, and informed consent.
This article is for educational purposes and does not constitute medical advice. Compounded medications, including those discussed here, are not FDA-approved for the indications described and should be used only under the direction of a qualified, licensed healthcare provider.
References
The studies cited here are available through PubMed and the publishers' websites. As always, I encourage curious readers to look at the abstracts themselves — bringing questions to your appointment is something I genuinely welcome.
[1] J. P. H. Wilding, R. L. Batterham, S. Calanna, et al., "Once-weekly semaglutide in adults with overweight or obesity," N. Engl. J. Med., vol. 384, no. 11, pp. 989–1002, Mar. 2021, https://doi.org/10.1056/nejmoa2032183
[2] A. M. Jastreboff, L. J. Aronne, N. N. Ahmad, et al., "Tirzepatide once weekly for the treatment of obesity," N. Engl. J. Med., vol. 387, no. 3, pp. 205–216, Jul. 2022, https://doi.org/10.1056/nejmoa2206038
[3] A. M. Lincoff, K. Brown-Frandsen, H. M. Colhoun, et al., "Semaglutide and cardiovascular outcomes in obesity without diabetes," N. Engl. J. Med., vol. 389, no. 24, pp. 2221–2232, Dec. 2023, https://doi.org/10.1056/nejmoa2307563
[4] Novo Nordisk, "Ozempic (semaglutide) injection: U.S. prescribing information," 2024. [Online]. Available: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/209637s029lbl.pdf
[5] V. R. Aroda, J. Rosenstock, Y. Terauchi, et al., "PIONEER 1: Randomized clinical trial of the efficacy and safety of oral semaglutide monotherapy in comparison with placebo in patients with type 2 diabetes," Diabetes Care, vol. 42, no. 9, pp. 1724–1732, Sep. 2019, https://doi.org/10.2337/dc19-0749
[6] R. Pratley, A. Amod, S. T. Hoff, et al., "Oral semaglutide versus subcutaneous liraglutide and placebo in type 2 diabetes (PIONEER 4): A randomised, double-blind, phase 3a trial," Lancet, vol. 394, no. 10192, pp. 39–50, Jul. 2019, https://doi.org/10.1016/s0140-6736(19)31271-1
[7] M. Davies, L. Færch, O. K. Jeppesen, et al., "Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): A randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial," Lancet, vol. 397, no. 10278, pp. 971–984, Mar. 2021, https://doi.org/10.1016/s0140-6736(21)00213-0
[8] Y. Liu, G. Song, D. Banov, et al. “Single-dose pharmacokinetics of sublingual semaglutide in rats”, Eur. J. Pharm. Sci., vol. 217, p. 107406, Feb. 2026, https://doi.org/10.1016/j.ejps.2025.107406
[9] U.S. Food and Drug Administration, "FDA clarifies policies for compounders as national GLP-1 supply begins to stabilize," 2025. [Online]. Available: https://www.fda.gov/drugs/drug-alerts-and-statements/fda-clarifies-policies-compounders-national-glp-1-supply-begins-stabilize