
Why Women Shouldn’t Have to Wait: The Case for Menopause Hormone Therapy During Perimenopause
Written and edited by Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Transdermal estradiol bypasses liver metabolism, which is a meaningful clinical advantage in perimenopause.
If you’re a woman in your late thirties or forties experiencing mood swings, brain fog, weight gain, insomnia, crushing fatigue, or a vanishing libido, you’ve probably been told one of two things: “It’s just stress,” or “You’re too young for menopause.”
And if you’re one of the persistent few who pushes back and asks about hormone therapy, you may hear something even more frustrating: “We have to wait until you’ve gone a full year without a period before we can treat you.”
As a clinician who works with women navigating the perimenopause transition every day, I want to be clear: that advice is outdated, and it is leaving millions of women suffering unnecessarily. The research is catching up to what many of us are seeing in practice—and what women have been telling us about their own bodies for years.
Understanding the Hormonal Storm of Perimenopause
Menopause is defined as 12 consecutive months without a menstrual period. But the transition leading up to it—perimenopause—can last anywhere from four to ten years, and it is where the most chaotic hormonal disruption occurs. The Stages of Reproductive Aging Workshop (STRAW+10) framework categorizes this transition into early and late phases, each with distinct hormonal signatures.
What makes perimenopause uniquely challenging is the unpredictability. The Study of Women’s Health Across the Nation (SWAN), a landmark longitudinal study following over 3,000 women through their menopausal transition, revealed that nearly 45% of women experienced a significant rise in estradiol levels before their final menstrual period—not the gradual decline most people assume. Estradiol can swing dramatically from one cycle to the next, sometimes reaching levels higher than a typical reproductive cycle and other times dropping to nearly undetectable levels.
Perimenopause is not simply “low estrogen.” It is a period of extreme hormonal variability—peaks and valleys of estradiol—that drives the symptoms women experience. This is most pronounced during mid-perimenopause.
This variability explains why women can feel pregnant one week and postmenopausal the next. It explains the unpredictable mood swings, the nights of drenching sweats followed by weeks of sleeping soundly, the brain fog that rolls in like weather. The SWAN data clearly demonstrated that late perimenopause—when women experience three or more months of amenorrhea—is the stage most strongly associated with vasomotor symptoms, depression, bone loss, and metabolic changes.
The Symptoms That Deserve Treatment Now
A Novel Approach: Symptom-Driven Hormone Therapy in Perimenopause
Here is what I am finding in clinical practice, and what I believe the research will increasingly support: women can learn to detect their own symptoms and treat with estradiol and/or progesterone as needed during the perimenopause transition.
Traditional guidelines focus on continuous daily therapy after menopause is established. But perimenopause is not postmenopause. The hormonal landscape is shifting, unpredictable, and highly individual. Because a woman’s own estradiol production can spike to excess one day and drop to undetectable the next, a rigid one-size-fits-all daily protocol may not serve every woman at every stage.
To my knowledge, using menopause hormone therapy on an as-needed basis—progesterone for sleep disruption, estradiol for hot flashes—has not been formally studied or recommended in guidelines. But many of my patients find meaningful relief using hormone therapy in this flexible, symptom-responsive manner.
My Clinical Prediction: In 20 years, when the evidence catches up, women will be empowered to detect their symptoms and treat with estradiol and/or progesterone as needed during the perimenopause transition—the way we now manage blood sugar with insulin or blood pressure with adjustable medications.
How Treatment May Evolve Across the Perimenopause Stages

Important Clinical Note: MHT Is Not Birth Control
Menopause hormone therapy does not suppress ovulation and should not be relied upon as contraception. Women in perimenopause can and do still ovulate—sometimes unpredictably—and pregnancy is possible until menopause is confirmed. If you are using MHT during perimenopause and are not seeking pregnancy, you need a reliable birth control plan in place. Discuss your contraceptive options with your clinician alongside any hormone therapy decisions. This is a conversation I have with every patient, because the hormones we use for symptom relief are at doses far too low to prevent pregnancy.
Why Transdermal Estradiol: The Divigel Advantage
In my practice, I have found that daily transdermal estradiol—specifically Divigel, an FDA-approved bioidentical estradiol gel—can provide significant relief for women in perimenopause. Transdermal delivery bypasses liver metabolism, which is a meaningful clinical advantage.
The ESTHER trial (Estrogen and Thromboembolism Risk), a multicenter case-cohort study, demonstrated no increased risk of venous thromboembolism with transdermal estrogen and micronized progesterone, compared to the elevated risk seen with oral estrogen formulations. Additional research confirms that transdermal estradiol avoids the prothrombotic effects of first-pass liver metabolism, does not elevate C-reactive protein, and maintains a more favorable lipid profile compared to oral formulations.
A network meta-analysis comparing transdermal estradiol gel preparations found that Divigel provided effective reduction in hot flush frequency and severity across its dose range, with the advantage of individualized dosing through its single-dose foil packet design. Divigel is available in doses ranging from 0.25 mg to 1.25 mg, allowing clinicians to tailor therapy to each patient’s needs.

Progesterone: Not Just Endometrial Protection
Micronized progesterone deserves far more attention in perimenopause care than it currently receives. Beyond its essential role in endometrial protection for women using estrogen therapy, progesterone has direct neurological effects that make it a powerful tool for one of perimenopause’s most debilitating symptoms: insomnia.
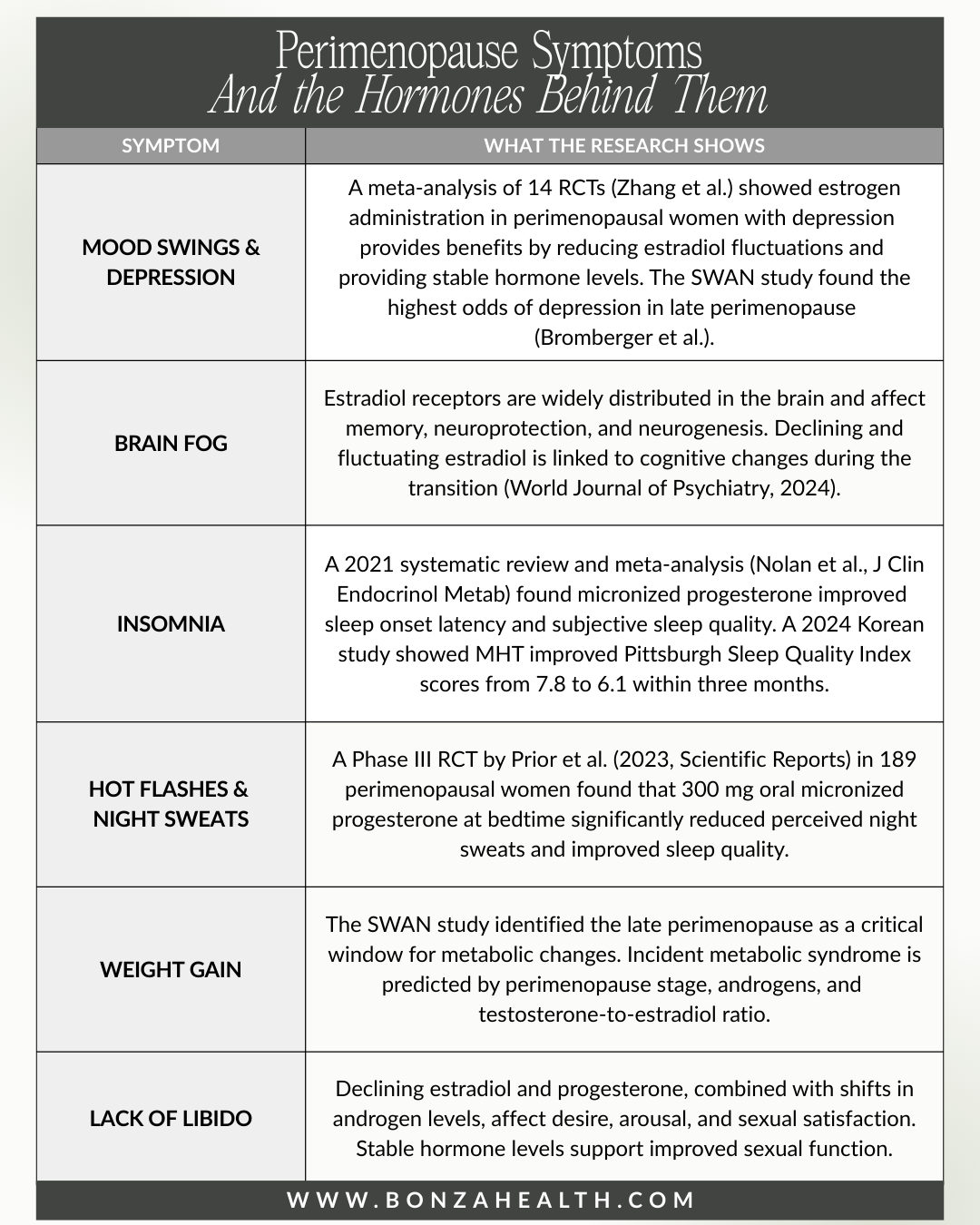
A 2021 systematic review and meta-analysis published in the Journal of Clinical Endocrinology & Metabolism (Nolan et al.) analyzed nine randomized controlled trials and found that micronized progesterone improved multiple sleep parameters measured by polysomnography, including total sleep time and sleep onset latency. Unlike benzodiazepines, micronized progesterone does not cause dependency, does not impair cognition, and does not disrupt normal sleep architecture.
A landmark Phase III Canadian RCT by Prior et al., published in Scientific Reports (2023), studied 189 perimenopausal women and found that 300 mg oral micronized progesterone at bedtime significantly reduced perceived night sweats and improved sleep quality. The study also noted decreased daytime vasomotor symptom intensity—a benefit that cannot be attributed solely to improved sleep.
Progesterone’s mechanism is physiological: when administered orally, it metabolizes into allopregnanolone, a neuroactive steroid that modulates GABA-A receptors—the same system targeted by many prescription sleep and anxiety medications, but without the dependency risks.

Dismantling the Fear: What the WHI Actually Showed
No discussion of menopause hormone therapy is complete without addressing the elephant in the room: the Women’s Health Initiative.
In 2002, the WHI published findings that appeared to show hormone therapy increased the risk of breast cancer, heart disease, and stroke. The results were widely publicized, and the FDA placed a black box warning—its strongest safety alert—on all estrogen-containing products. Use of hormone therapy among postmenopausal women dropped by nearly 50% almost overnight. Millions of women suffered unnecessarily for over two decades because of this single study.
Here is what most people do not know: the original interpretation was deeply flawed. The average age of WHI participants was 63 years—over a decade past the typical age of menopause onset. The study used conjugated equine estrogens derived from pregnant horse urine, combined with a synthetic progestin (medroxyprogesterone acetate)—formulations that are not equivalent to the bioidentical 17β-estradiol and micronized progesterone used in modern practice. And the study was designed to evaluate disease prevention in older women, not symptom treatment in younger women transitioning through menopause.
In November 2025, the FDA officially removed the black box warning from estrogen-containing hormone therapy products, citing that the original risks were overstated. Updated labeling now acknowledges that women who initiate HRT within 10 years of menopause onset may experience reduced all-cause mortality, up to 50% reduction in heart attack risk, 35% lower risk of Alzheimer’s, and 50–60% reduction in bone fractures.
A 2024 study published in Menopause, The Journal of the Menopause Society, examined outcomes across 40 different hormonal therapies in women over 65 and found that estrogen-only therapy was associated with a 19% reduction in mortality and significant risk reductions for breast cancer, lung cancer, colorectal cancer, heart failure, and dementia. The reanalysis of WHI data showed estrogen-only therapy was associated with a lower risk of breast cancer compared to placebo—directly contradicting the original narrative.
An Honest Conversation: How Little We Truly Know
Despite these encouraging findings, I want to be transparent: we still have significant gaps in our understanding of long-term hormone therapy outcomes. Most studies have followed women for five to twenty years. We have limited data on outcomes beyond that window, and almost no prospective research on the flexible, symptom-driven approach I am describing.
What I can tell you is what I observe in practice. I have a patient in her 80s who has been on long-term oral estradiol therapy. She does not look or act a day over 60. Her cognitive function, bone density, skin integrity, energy, and overall vitality are remarkable. Is this a study? No. But it is a data point that deserves attention, and it aligns with the emerging evidence suggesting that the benefits of hormone therapy may extend well beyond the traditional “10-year window.”
The 2024 Lancet Diabetes & Endocrinology review proposed that current guidelines limiting MHT initiation to within 10 years of menopause need revision to be more inclusive, arguing that many women outside these chronological limits could benefit from therapy.

Bridging Two Worlds: The Menopause Society and Functional Medicine
I believe there is tremendous value in bridging the perspectives of The Menopause Society and the Institute for Functional Medicine.
The Menopause Society takes a rigorous, evidence-based approach and has been instrumental in shifting the conversation around MHT safety. Their updated position statement supports individualized hormone therapy as the most effective treatment for vasomotor symptoms and emphasizes shared decision-making between clinicians and patients.
The Institute for Functional Medicine views these hormone changes through a broader lens—considering how nutrition, gut health, stress, environmental toxins, sleep, and lifestyle factors interact with hormonal shifts. Functional medicine recognizes that hormone therapy is one tool within a comprehensive approach to health optimization, and that the terrain in which hormones operate matters as much as the hormones themselves.
These are not opposing philosophies. The best care for women in perimenopause honors both: using the strongest available evidence to guide hormone prescribing, while also addressing the root causes and lifestyle factors that influence how a woman experiences this transition. Not every woman in perimenopause needs hormone therapy, and not every woman who needs hormone therapy needs the same protocol.

The Bottom Line: You Deserve Treatment Now
If you are in perimenopause and experiencing symptoms that are affecting your quality of life, you should not have to wait for an arbitrary milestone to access treatment. The science supports early intervention. The FDA has removed the black box warning. The Menopause Society endorses individualized therapy. And clinical experience is showing us that flexible, symptom-driven approaches may serve many women better than rigid one-size-fits-all protocols.
My approach may be novel. I believe it is somewhat revolutionary. And I predict that in 20 years, when the evidence catches up, this will be the standard of care. Until then, I will continue to listen to my patients, stay grounded in the best available science, and advocate fiercely for women’s right to feel well during every stage of their lives.
If you’re ready to explore whether menopause hormone therapy might be right for you during perimenopause, I invite you to schedule a consultation at Bonza Health.

Book your 50-minute consultation with Dr. Bonza to receive 12 months of menopause care
References
1. Randolph JF et al. “Trajectory clustering of estradiol and FSH during the menopausal transition among women in SWAN.” J Clin Endocrinol Metab. 2012;97(8):2872–2880.
2. Nolan BJ, Liang B, Cheung AS. “Efficacy of micronized progesterone for sleep: a systematic review and meta-analysis of RCT data.” J Clin Endocrinol Metab. 2021;106(4):e942–e951.
3. Prior JC, Cameron A, Fung M, et al. “Oral micronized progesterone for perimenopausal night sweats and hot flushes: a Phase III Canada-wide RCT.” Scientific Reports. 2023;13:9082.
4. Zhang M, et al. “Meta-analysis of 14 RCTs: estrogen administration in perimenopausal women with depression.” (As cited in World J Psychiatry, 2024.)
5. Canonico M, et al. “ESTHER Study: Hormone therapy and VTE risk.” Circulation. 2007;115(7):840–845.
6. Derzko C, et al. “Comparative efficacy and safety of estradiol transdermal preparations (Divigel vs. Estrogel).” Menopause. 2016;23(3):294–303.
7. Simon JA, et al. “Transdermal estradiol gel 0.1% (Divigel) for vasomotor symptoms.” Menopause. 2007;14(5):863–872.
8. Manson JE, et al. “Menopausal hormone therapy and health outcomes: WHI randomized trials.” JAMA. 2013;310(13):1353–1368.
9. Manson JE, Crandall CJ, Rossouw JE, et al. “The WHI randomized trials and clinical practice: A review.” JAMA. 2024. doi:10.1001/jama.2024.6542.
10. FDA/HHS. “FDA Initiates Removal of Black Box Warnings from Menopausal HRT Products.” November 10, 2025.
11. Lozza-Fiacco S, et al. “Estradiol variability and perimenopausal anxiety/anhedonia.” (As cited in PMC, 2024.)
12. Santoro N, et al. “The menopause transition and women’s health at midlife: SWAN progress report.” Menopause. 2019;26(10):1213–1227.
13. Cagnacci A, Venier M. “The controversial history of hormone replacement therapy.” Medicina. 2019;55(9):602.
14. Mukherjee K, et al. “Update on MHT: Current indications and unanswered questions.” Clinical Endocrinology. 2025. doi:10.1111/cen.15211.