
The Silent Thief: Why We Must Advocate for Earlier DEXA Screening in Women
Written and edited by Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Osteoporosis does not begin at menopause. It begins well before, during the perimenopausal years when women still have menstrual cycles.
Osteoporosis is often called “the silent thief” because it steals bone density without warning — no pain, no symptoms, and no red flags — until a fracture occurs. Despite affecting over 200 million people worldwide [1] and causing more than 8.9 million fractures annually [2], our screening guidelines remain reactive rather than proactive, particularly for women under 65 who carry significant risk factors. As clinicians, we must ask ourselves: are we waiting too long to look?
What the Current Guidelines Say
The U.S. Preventive Services Task Force (USPSTF) updated its osteoporosis screening recommendations in January 2025, reaffirming that universal screening with dual-energy X-ray absorptiometry (DEXA) is recommended for all women aged 65 and older (Grade B recommendation) [3]. For postmenopausal women younger than 65, the USPSTF recommends screening only for those deemed to be at increased risk based on clinical risk assessment tools such as FRAX [3].
The American College of Obstetricians and Gynecologists (ACOG) echoes a similar position, recommending bone mineral density (BMD) screening beginning at age 65 for all women and selective screening for younger women with elevated risk [3]. The American Academy of Family Physicians goes further still, specifically recommending against DEXA screening in women younger than 65 who have no identified risk factors [3].
What is notably absent from these guidelines is any formal recommendation to screen premenopausal or perimenopausal women — even those with strong family histories, multiple pregnancies, or other well-documented risk factors. The implicit assumption is that osteoporosis is a disease of the elderly postmenopausal woman. As a growing body of evidence demonstrates, this assumption is dangerously wrong.
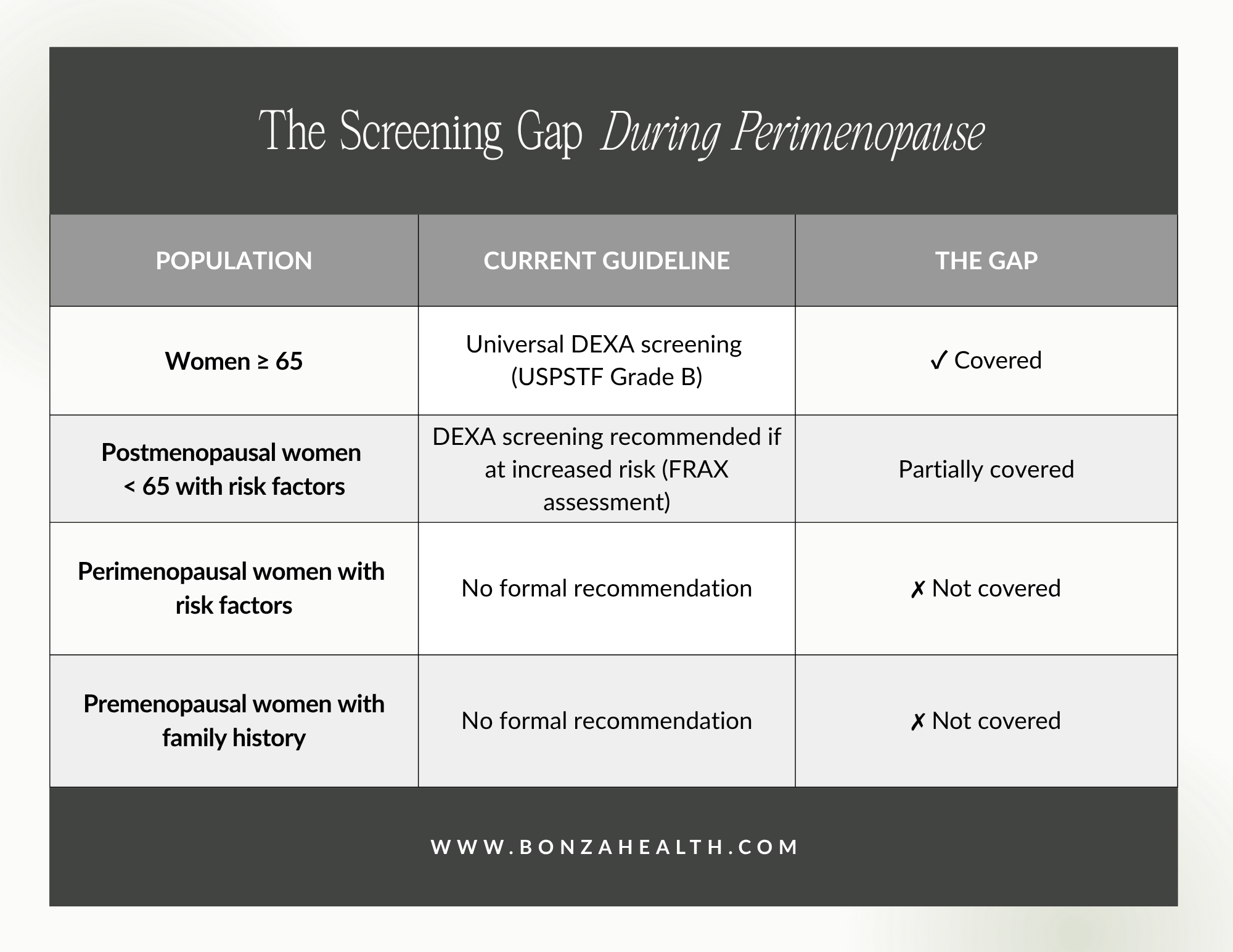
Current DEXA screening guidelines leave millions of at-risk women unscreened. Here’s what the guidelines say — and what’s missing.
Source: USPSTF 2025 Recommendation Statement [3]
The Problem: By the Time We Screen, It’s Already Too Late
The age-adjusted prevalence of osteoporosis among community-dwelling U.S. residents aged 50 and older is 12.6%, and among women 65 and older, that number jumps to 27.1% [3]. But these figures only capture those who have been screened. A landmark finding from the National Osteoporosis Risk Assessment (NORA) study revealed that 7.2% of over 200,000 assessed postmenopausal women had undiagnosed osteoporosis, placing them at a four-fold increased risk of fracture without ever knowing it [4]. Low bone mineral density does not cause pain or any other symptoms, and without screening, individuals often do not learn they have osteoporosis until after a fracture has already occurred [5].
The data from the Study of Women’s Health Across the Nation (SWAN) are even more sobering: 10-year cumulative bone loss averaged 9.1% at the femoral neck and 10.6% at the lumbar spine during the menopausal transition [6]. This bone loss is not exclusive to the postmenopausal period.
Longitudinal research has demonstrated that women in the perimenopausal transition lose trabecular bone at a rapid rate, even when estrogen levels are intermittently high or within normal ranges [7]. Indeed, each doubling of follicle-stimulating hormone (FSH) levels during the menopause transition is associated with an additional 0.3% annual decline in BMD at the femoral neck and lumbar spine [8]. Bone loss accelerates markedly during late perimenopause, with average annual declines of approximately 2.5% in the lumbar spine and 1.7% in the femoral neck reported during the time surrounding the final menstrual period [9].
These findings shatter a common misconception: osteoporosis does not begin at menopause. It begins well before, during the perimenopausal years when women still have menstrual cycles.
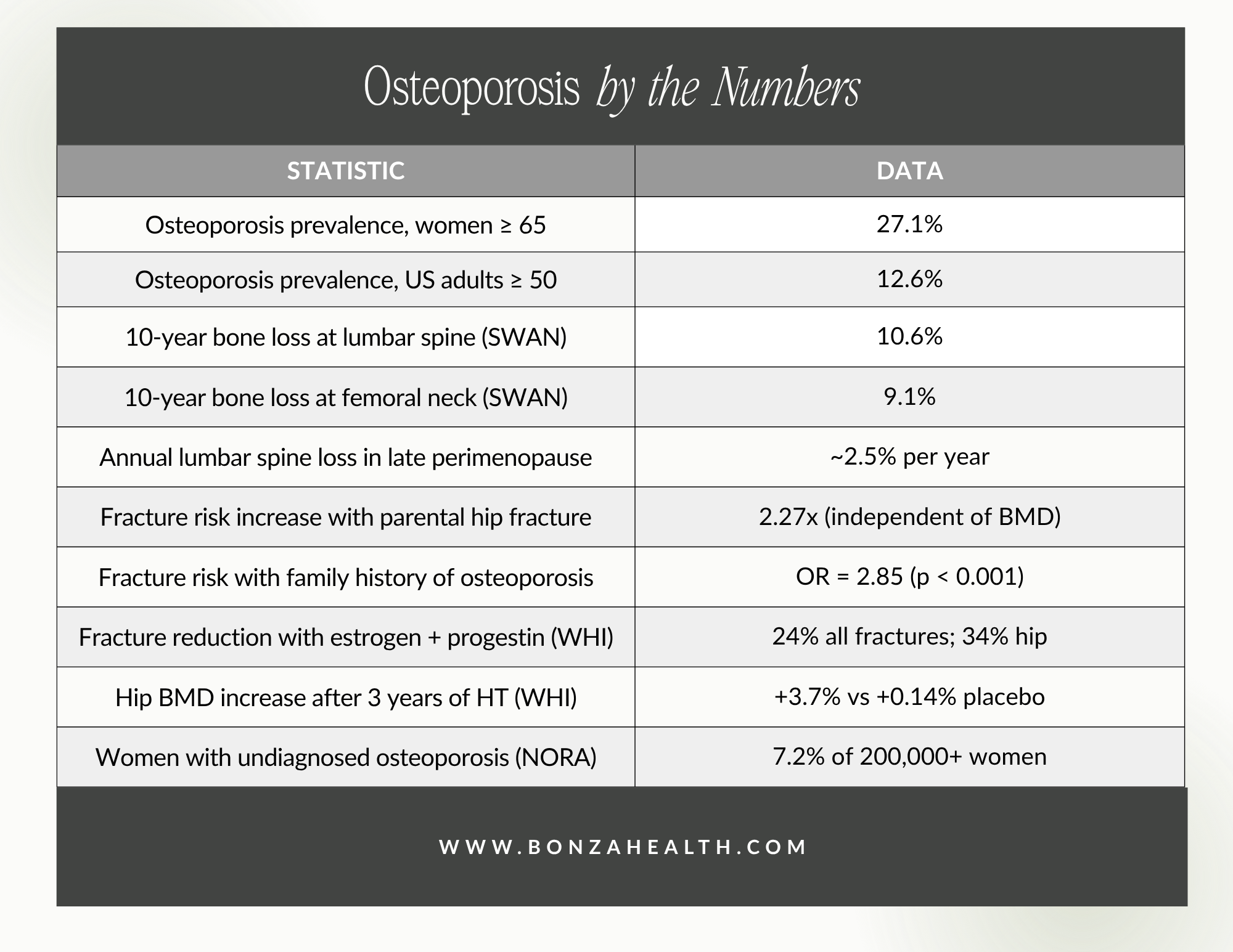
Osteoporosis doesn’t wait until 65. Here are the numbers your doctor may not be telling you.
Sources: USPSTF 2025 [3]; SWAN [6]; Kanis et al. 2004 [11]; Dobre et al. 2021 [13]; Cauley et al. 2003 [17]
When Family History Speaks, We Must Listen
Osteoporosis is a polygenic disorder with a strong genetic component. Twin and family studies have consistently shown that genetic factors play a critical role in regulating bone mineral density, skeletal geometry, bone turnover, and ultimately fracture risk [10]. A large meta-analysis of over 34,000 men and women across seven prospective cohorts found that a parental history of hip fracture conferred a significant and BMD-independent increase in the risk of both osteoporotic fracture (RR = 1.54; 95% CI: 1.25–1.88) and hip fracture (RR = 2.27; 95% CI: 1.47–3.49) [11]. Crucially, this increased risk persisted even after adjusting for bone mineral density, indicating that family history captures fracture susceptibility through mechanisms beyond BMD alone — including inherited differences in bone microarchitecture, geometry, and turnover [11].
Population-based studies have further confirmed a strong familial association of bone mineral density between parents and offspring, with the relationship persisting after controlling for lifestyle and environmental factors [12]. In one analysis of women with a positive family history of osteoporosis, the presence of family history significantly increased fracture prevalence (37% vs 17%, p<0.001; OR = 2.85), and notably, fractures occurred at higher (better) T-scores and Z-scores than in the general population [13]. This means that women with a family history may fracture at bone density levels that would be considered “safe” by conventional thresholds, underscoring the limitation of relying solely on age-based screening triggers.

Family history of osteoporosis, multiparity, low body weight, smoking, prolonged breastfeeding, early perimenopause, and other established risk factors should be sufficient justification for DEXA screening at any age.
A Case That Changed My Practice
I recently cared for a 42-year-old woman — a mother of five who was still having regular menstrual cycles. Her mother had suffered multiple osteoporotic fractures. Concerned about her own bone health, this patient went to her primary care provider and requested a DEXA scan. She was declined. The reason? She was “too young.”
This answer, while aligned with a strict reading of existing guidelines, was a missed opportunity. Using the ICD-10 diagnosis code Z82.62 — family history of osteoporosis — we were able to get her DEXA scan covered by insurance. The results were alarming: she already had osteoporosis at age 42, while still menstruating.
Had we not advocated for this screening, she would have continued losing bone density silently for potentially another 20 years before reaching the age threshold for routine screening. By that time, she could have already experienced the same devastating fractures as her mother. Instead, we identified her disease early and were able to intervene.
This case is not an anomaly. It is a wake-up call.
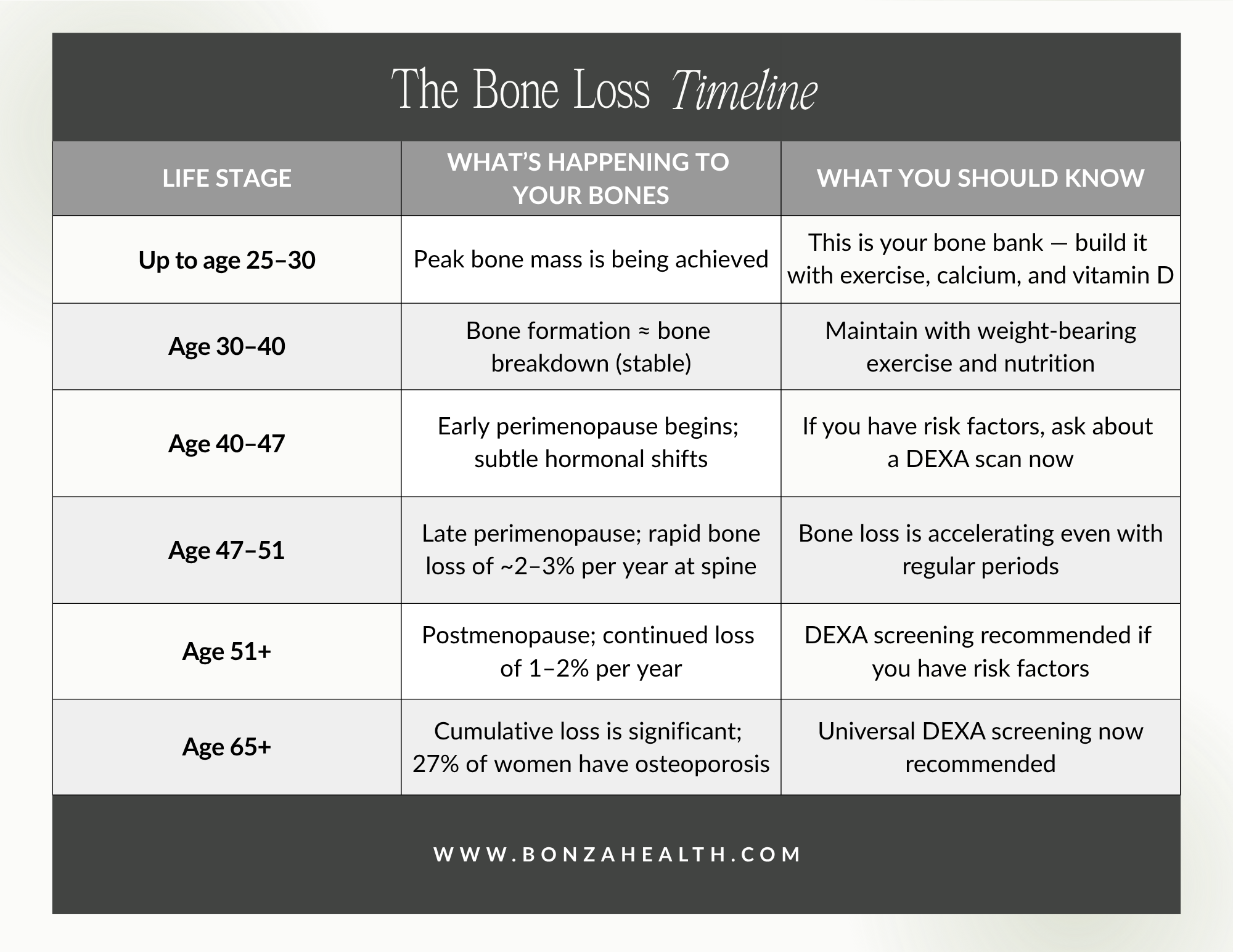
Your bones start changing long before menopause. Here’s a timeline every woman should see.
Sources: SWAN [6]; Gass et al. 2012 [7]; Harlow et al. 2011 [9]; USPSTF 2025 [3]
Perimenopause: The Overlooked Window of Vulnerability
Many clinicians and patients alike assume that bone loss is primarily a postmenopausal concern, but the perimenopausal transition represents a critical and underappreciated window of skeletal vulnerability. During perimenopause — which typically begins at an average age of 47 — fluctuating hormones and rising FSH levels initiate a cascade of changes in bone remodeling [8], [9]. Bone turnover markers show their steepest increases during the menopause transition rather than after it [7]. Longitudinal evidence confirms that BMD loss accelerates during late perimenopause, with rates comparable to or exceeding those seen in the early postmenopausal years [9].
Multiple pregnancies may compound this risk. Pregnancy and breastfeeding are associated with major changes in maternal calcium homeostasis, bone metabolism, and the rate of bone remodeling [14]. While the relationship between parity and postmenopausal bone density is complex and debated, several studies have found that grand multiparity is associated with lower bone mineral density at the femoral neck and degraded trabecular bone patterns [14], [15]. One study reported that femoral bone mineral density significantly decreased as the number of deliveries increased [16]. Extended breastfeeding, which creates an estrogen-deficient state, may further contribute to microstructural deterioration with uncertain long-term reversibility [14].
For women like my patient — perimenopausal, multiparous, and with a strong family history — the convergence of genetic susceptibility, reproductive history, and hormonal transition creates a perfect storm for accelerated bone loss. And yet, under current guidelines, these women are invisible to the screening system.

Many clinicians and patients alike assume that bone loss is primarily a postmenopausal concern, but the perimenopausal transition represents a critical and underappreciated window of skeletal vulnerability.
The Protective Power of Early Estrogen Therapy
The evidence supporting estrogen’s role in bone health is robust and long-standing. The Women’s Health Initiative (WHI), the largest randomized controlled trial of hormone therapy in postmenopausal women, demonstrated that estrogen plus progestin reduced the risk of all fractures by 24%, including a 34% reduction in hip and clinical vertebral fractures [17]. Total hip BMD increased 3.7% after three years of treatment compared with just 0.14% in the placebo group [17]. In the estrogen-alone arm of the WHI, conjugated equine estrogen also significantly reduced fracture risk and increased BMD in hysterectomized postmenopausal women [18]. Remarkably, the fracture-protective effect was consistent across all subgroups, regardless of age, BMI, smoking status, fracture history, or baseline bone density [17].
Menopause hormone therapy (MHT) is the only anti-osteoporotic therapy that has demonstrated efficacy in reducing fracture risk regardless of the baseline level of risk — even in women at low risk for fracture [19]. It prevents bone loss, preserves bone microarchitecture, and reduces the risk of fracture at all skeletal sites by approximately 20–40% [19]. Beyond its antiresorptive properties, estrogen uniquely attenuates the inflammatory bone microenvironment that accompanies estrogen deficiency — an effect not achieved by other antiresorptive therapies [20].
A meta-analysis of transdermal estrogen delivery found that one to two years of transdermal estrogen therapy significantly increased lumbar spine BMD by 3.4% at one year and 3.7% at two years compared to baseline [4]. Low-dose and transdermal formulations appear to carry a more favorable safety profile with respect to breast cancer, coronary artery disease, venous thromboembolism, and endometrial hyperplasia compared to standard-dose oral regimens [21]. This has led to an emerging consensus that there may be a “window of opportunity” in the early postmenopausal years (within 10 years of menopause onset) during which hormone therapy is both maximally effective for bone health and safest from a cardiovascular and oncologic perspective [22].
For women identified early — particularly those in perimenopause with risk factors — timely initiation of estrogen therapy can prevent the rapid, irreversible bone loss that characterizes the menopausal transition. As one group of researchers summarized: screening perimenopausal women at risk should identify osteopenic women early, before the accelerated bone loss of estrogen deficiency causes further irreversible erosion in bone density [23].
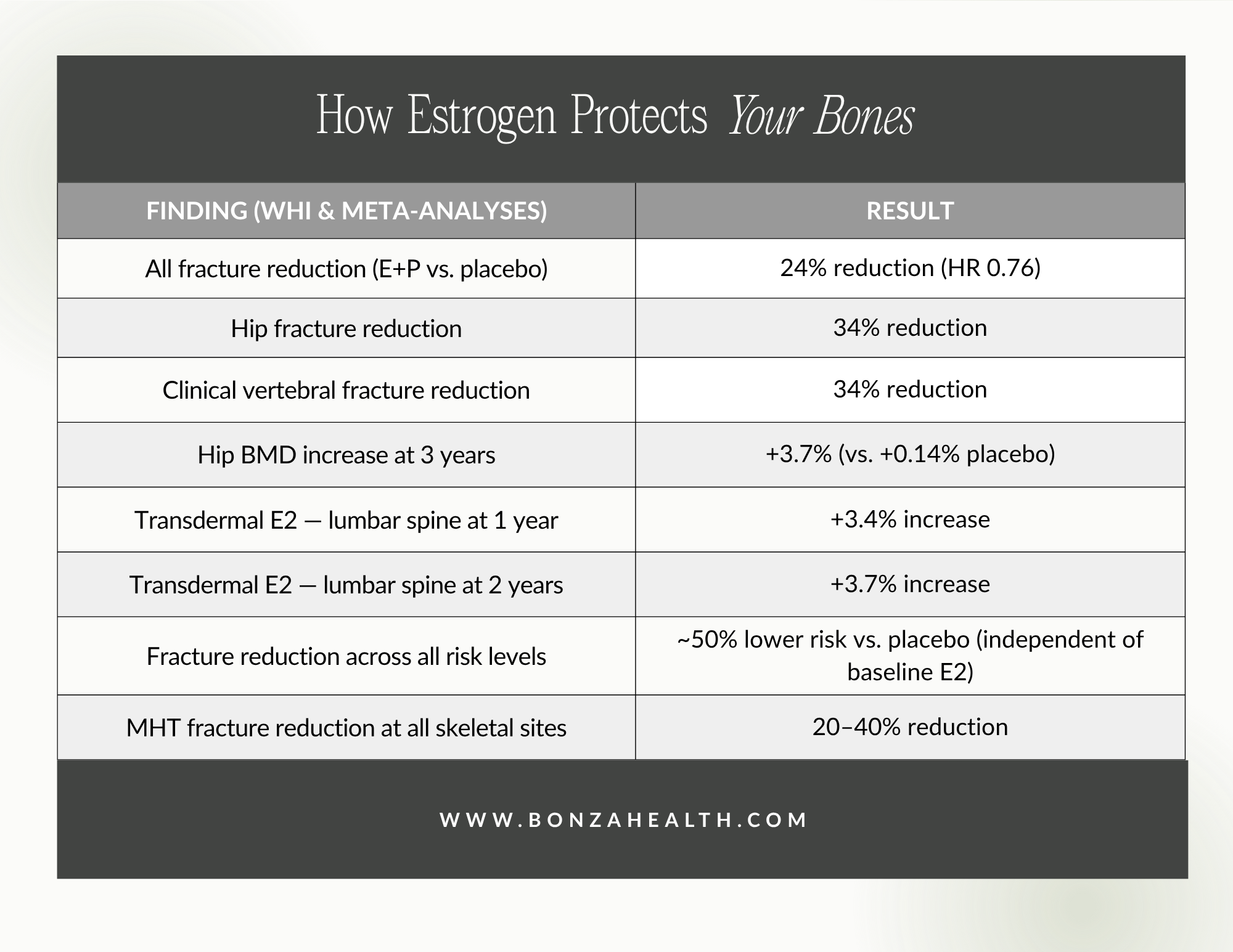
Estrogen isn’t just about hot flashes. It’s the most powerful bone protector we have.
Sources: Cauley et al. 2003 [17]; Jackson et al. 2006 [18]; Zhou et al. 2017 [4]; Stevenson et al. 2021 [19]
A Call to Action: Rethinking Our Approach to Screening
The current screening paradigm leaves too many women behind. While guidelines appropriately recommend universal screening at age 65 and risk-based screening for postmenopausal women under 65, they do not adequately address the needs of premenopausal and perimenopausal women with identifiable risk factors. Family history of osteoporosis, multiparity, low body weight, smoking, prolonged breastfeeding, early perimenopause, and other established risk factors should be sufficient justification for DEXA screening at any age.
For Clinicians
Do not dismiss younger women who request bone density screening, particularly those with a family history of fractures or osteoporosis. The ICD-10 code Z82.62 (family history of osteoporosis) is a valid, billable diagnostic code that can support insurance coverage for DEXA scans in women who do not yet meet age-based screening criteria. Screening at-risk women earlier allows for timely intervention — with estrogen therapy, bisphosphonates, lifestyle modifications, or a combination thereof — before irreversible bone loss occurs.
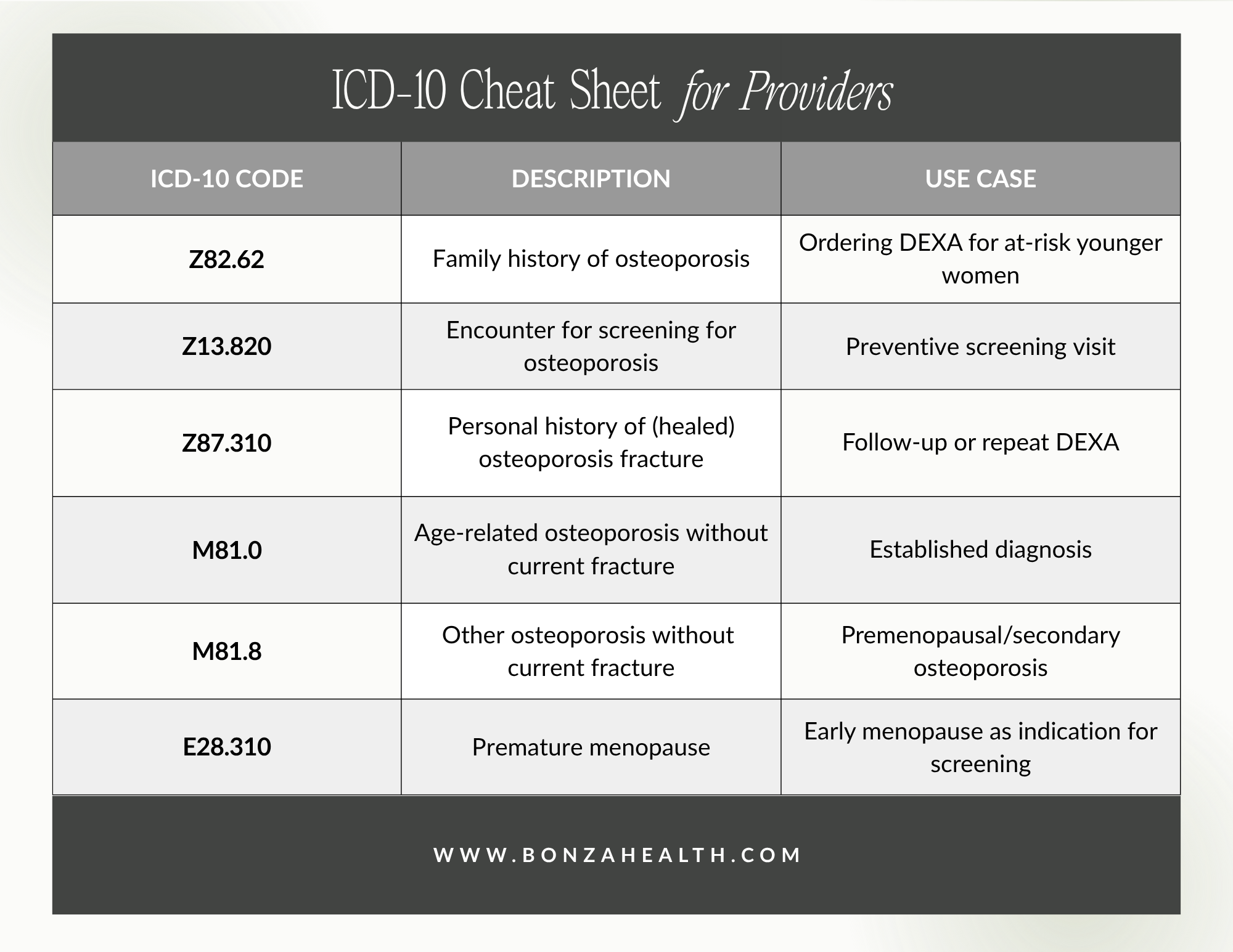
Providers: Don’t let insurance be the reason a woman doesn’t get screened. These codes can help.
For Patients
If your mother, grandmother, or other close relative has had osteoporotic fractures or been diagnosed with osteoporosis, speak up. Ask your provider about a DEXA scan. If you are told you are “too young,” know that risk-based screening is supported by USPSTF guidelines and that a documented family history can make you eligible. Your bone health is worth advocating for.
For the Medical Community
We need prospective studies examining the impact of earlier screening strategies on fracture prevention in at-risk premenopausal and perimenopausal women. We also need updated guidelines that explicitly address perimenopause as a period of heightened skeletal vulnerability and that recognize family history as a standalone indication for screening, independent of age.
Osteoporosis is a preventable tragedy when caught early. We have effective diagnostic tools. We have effective therapies. What we lack is the clinical will to use them sooner.
My 42-year-old patient with five children and a mother riddled with fractures is proof that osteoporosis does not wait until we are ready to look for it. Neither should we.

Book your evaluation with Dr. Bonza
References
[1] S. Sözen, L. Özışık, and N. Ç. Başaran, “An overview and management of osteoporosis,” Eur. J. Rheumatol., vol. 4, no. 1, pp. 46–56, 2017. PubMed PMID: 28293453
[2] O. Johnell and J. A. Kanis, “An estimate of the worldwide prevalence and disability associated with osteoporotic fractures,” Osteoporos. Int., vol. 17, no. 12, pp. 1726–1733, 2006. PubMed PMID: 16983459
[3] US Preventive Services Task Force et al., “Screening for osteoporosis to prevent fractures: US Preventive Services Task Force recommendation statement,” JAMA, vol. 333, no. 6, pp. 498–508, 2025. PubMed PMID: 39808425
[4] J. Zhou et al., “The effects of transdermal estrogen delivery on bone mineral density in postmenopausal women: A meta-analysis,” Medicine, vol. 96, no. 19, e6839, 2017. PMC5423263
[5] E. S. Siris et al., “Bone mineral density thresholds for pharmacological intervention to prevent fractures,” Arch. Intern. Med., vol. 164, no. 10, pp. 1108–1112, 2004. PubMed PMID: 15159268
[6] G. A. Greendale et al., “Bone mineral density loss in relation to the final menstrual period in a multiethnic cohort: Results from SWAN,” J. Bone Miner. Res., vol. 27, no. 1, pp. 111–118, 2012. PubMed PMID: 21976367
[7] M. L. Gass et al., “Bone loss in premenopausal, perimenopausal and postmenopausal women: Results of a prospective observational study over 9 years,” Climacteric, vol. 15, no. 6, pp. 563–570, 2012. PubMed PMID: 22443333
[8] A. Stefanska et al., “The role of follicle-stimulating hormone in bone loss during menopause transition: A narrative review,” Endocrines, vol. 6, no. 4, Art. no. 54, 2025.
[9] S. D. Harlow et al., “Bone and the perimenopause,” Obstet. Gynecol. Clin. North Am., vol. 38, no. 3, pp. 503–517, 2011. PMC3920744
[10] S. H. Ralston, “Role of genetic factors in the pathogenesis of osteoporosis,” J. Endocrinol., vol. 166, no. 2, pp. 235–245, 2000. PubMed PMID: 10927613
[11] J. A. Kanis et al., “A family history of fracture and fracture risk: A meta-analysis,” Bone, vol. 35, no. 5, pp. 1029–1037, 2004. PubMed PMID: 15542027
[12] H. S. Choi et al., “Strong familial association of bone mineral density between parents and offspring: KNHANES 2008-2011,” Osteoporos. Int., vol. 28, no. 3, pp. 955–964, 2017. PubMed PMID: 27747365
[13] D. Dobre, A. Barbu, et al., “Family history — BMD independently — influences fracture risk,” Acta Medica Transilvanica, vol. 26, no. 4, pp. 62–65, 2021. PMC9206152
[14] N. Panahi et al., “Grand multiparity associations with low bone mineral density and degraded trabecular bone pattern,” Bone Rep., vol. 14, Art. no. 101071, 2021. PubMed PMID: 33997148
[15] S. Sahin Ersoy et al., “Is grand multiparity a risk factor for the development of postmenopausal osteoporosis?,” Clin. Interv. Aging, vol. 13, pp. 505–508, 2018. PubMed PMID: 29636605
[16] B. K. Sharma et al., “Effect of multiparity and prolonged lactation on bone mineral density,” J. Menopausal Med., vol. 22, no. 3, pp. 161–166, 2016. PubMed PMID: 28119896
[17] J. A. Cauley et al., “Effects of estrogen plus progestin on risk of fracture and bone mineral density: The WHI randomized trial,” JAMA, vol. 290, no. 13, pp. 1729–1738, 2003. PubMed PMID: 14519707
[18] R. D. Jackson et al., “Effects of conjugated equine estrogen on risk of fractures and BMD in postmenopausal women with hysterectomy: Results from the WHI,” J. Bone Miner. Res., vol. 21, no. 6, pp. 817–828, 2006. PubMed PMID: 16753012
[19] J.-C. Stevenson et al., “Menopausal hormone therapy for the management of osteoporosis,” Climacteric, vol. 24, no. 6, pp. 513–519, 2021. PubMed PMID: 34119418
[20] R. Marjoribanks et al., “Update on menopausal hormone therapy for fracture prevention,” Curr. Osteoporos. Rep., vol. 17, no. 6, pp. 465–473, 2019.
[21] A. M. Cheung et al., “Estrogen therapy for osteoporosis in the modern era,” Clin. Obstet. Gynecol., vol. 61, no. 3, pp. 481–488, 2018. PubMed PMID: 29520604
[22] A. V. Schwartz et al., “Revisiting estrogen: Efficacy and safety for postmenopausal bone health,” Int. J. Women’s Health, vol. 2, pp. 263–274, 2010. PMC2957171
[23] R. A. Lobo, “Bone metabolism and the perimenopause: Overview, risk factors, screening, and osteoporosis preventive measures,” Obstet. Gynecol. Clin. North Am., vol. 29, no. 3, pp. 495–510, 2002. PubMed PMID: 12353670