
Your Body in Transition: A System-by-System Guide to Perimenopause
Written and edited by Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Perimenopause may start earlier than you think
Yesterday, a patient in her early forties sat across from me, describing something she had never experienced before: her heart would suddenly race for no apparent reason, jolting her awake at 2 a.m. She could not fall back asleep. She felt foggy at work. She wondered if something was seriously wrong.
Nothing was wrong with her heart. What she was experiencing were some of the earliest signals of perimenopause.
Perimenopause May Start Earlier Than You Think
Perimenopause is the transitional window leading up to menopause, the point at which your ovaries stop releasing eggs and menstrual periods cease permanently. While most women associate menopause with their fifties, the transition often begins much earlier. Research shows that perimenopause can start in the early forties and, for some women, even in the late thirties [1]. The Stages of Reproductive Aging Workshop (STRAW+10) criteria, the gold standard for classifying reproductive aging, divide this transition into distinct phases: early perimenopause, mid-to-late perimenopause, and the final menstrual period [2].
What makes this transition so confusing is that its effects extend far beyond irregular periods. Fluctuating and declining estrogen, progesterone, and testosterone impact virtually every organ system in the body. Your sleep architecture changes. Your cardiovascular system responds differently to stress. Your joints ache for reasons that imaging cannot explain. Your bladder behaves unpredictably. Your ability to recall a word you used yesterday vanishes mid-sentence.
The purpose of this blog is to walk you through the major body systems affected by perimenopause and to show you what to expect at each phase. My hope is that by understanding these changes, you will feel empowered rather than frightened, and that you will recognize the signals your body is sending you as it moves through this natural, but sometimes disorienting, transition.
Perimenopause is the transitional window leading up to menopause
Understanding the Phases: The STRAW+10 Framework
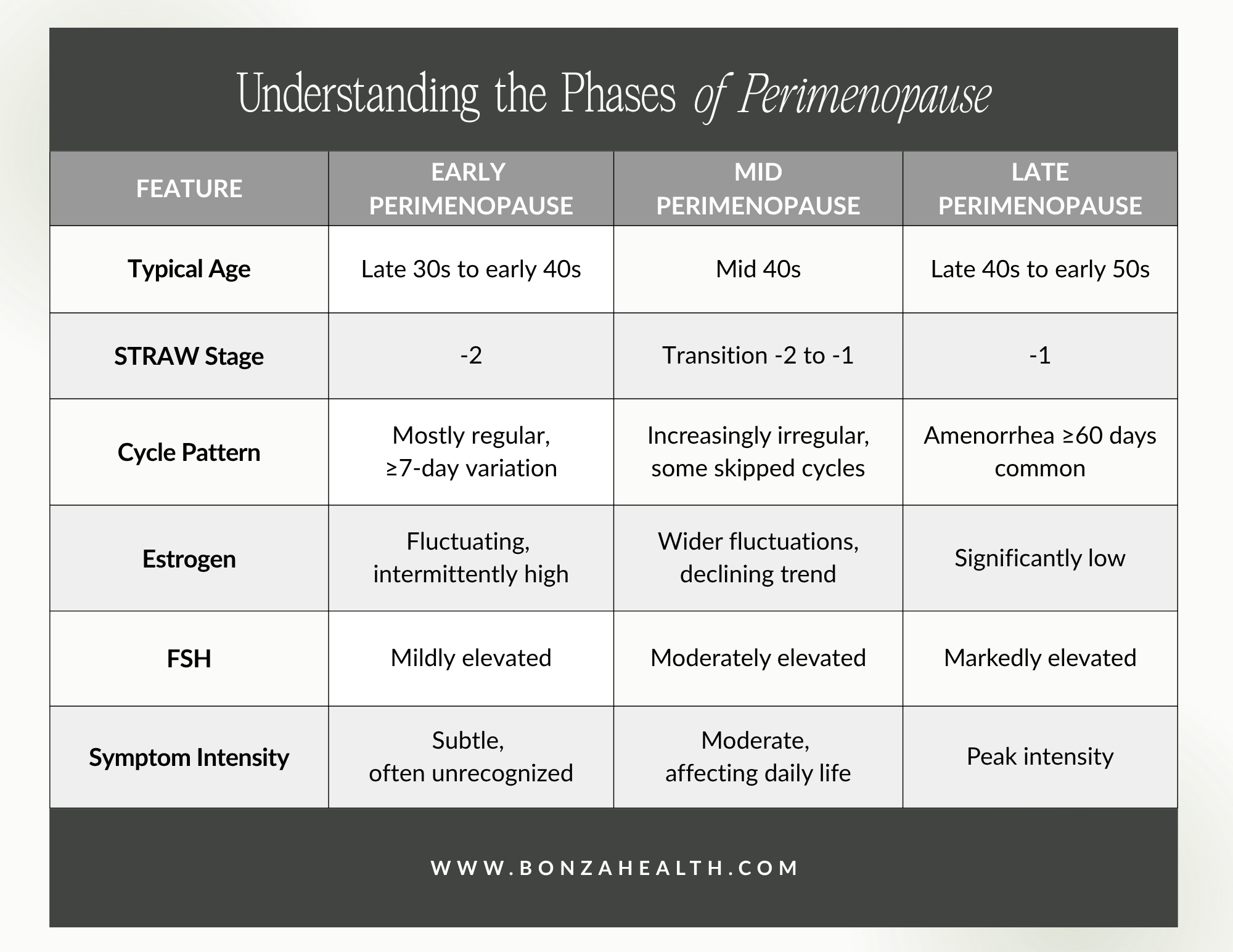
The STRAW+10 staging system is the internationally recognized framework for describing reproductive aging [2]. For the purposes of this blog, I have simplified the stages into three clinically meaningful phases:
Early Perimenopause (STRAW Stage -2): Cycles remain mostly regular but may begin to vary in length by seven or more days. Hormone levels start to fluctuate. Subtle symptoms may emerge. This phase often begins in the late thirties to early forties.
Mid Perimenopause (Transition between -2 and -1): Cycle variability increases. Some months may be skipped entirely. Symptoms become more noticeable and affect daily function. This typically occurs in the mid-forties.
Late Perimenopause (STRAW Stage -1): Periods of amenorrhea lasting 60 days or more become common. Estrogen levels drop significantly. Symptoms tend to peak in frequency and intensity. This phase usually occurs in the late forties to early fifties, ending with the final menstrual period.
Understanding the phases of perimenopause
1. Menstrual Cycle Changes
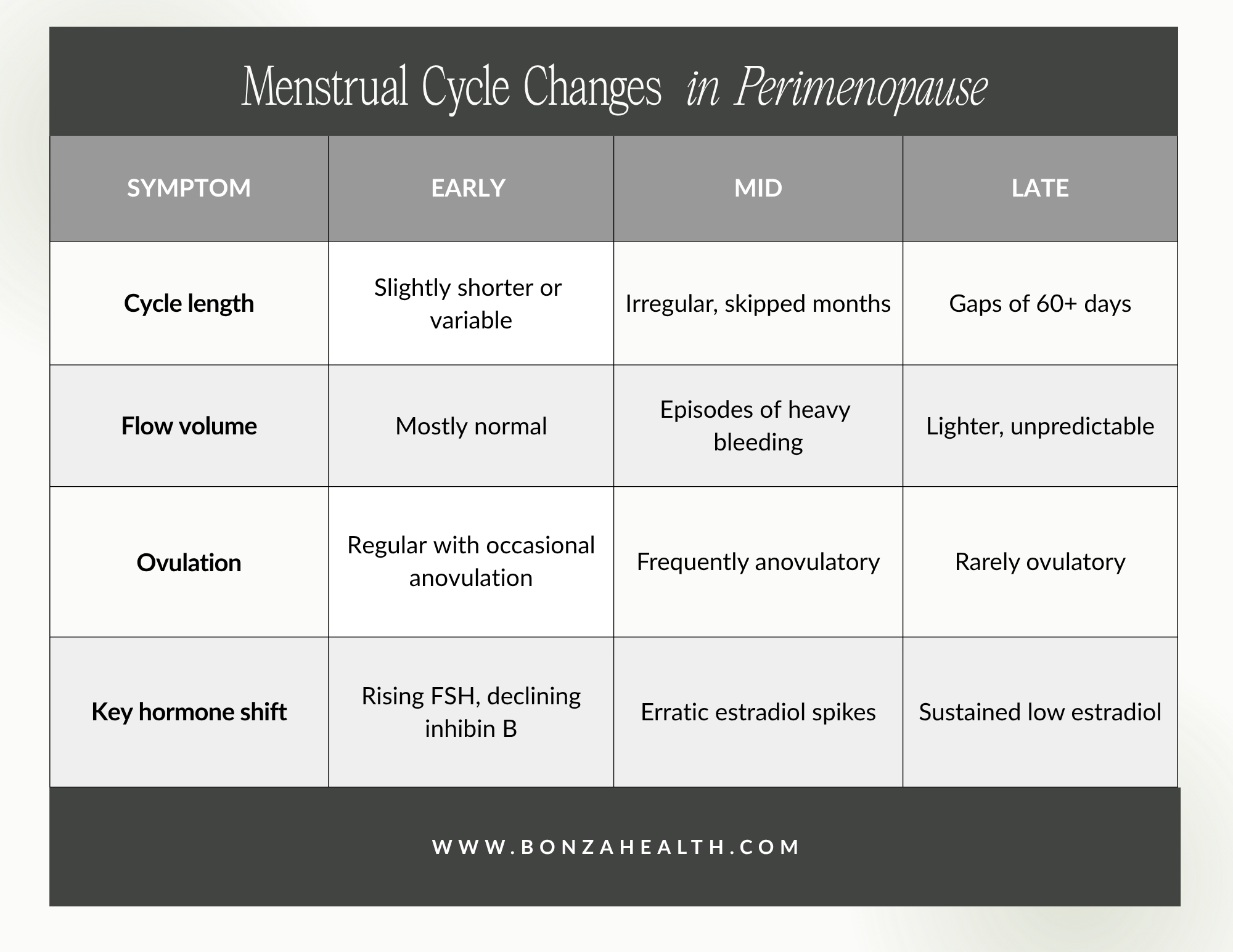
The menstrual cycle is often the first system to signal the onset of perimenopause. Changes in cycle length, flow volume, and regularity reflect the underlying hormonal shifts happening in the ovaries.
Early Perimenopause
During early perimenopause, cycles may remain largely predictable, but subtle shifts begin to appear. You might notice that your cycle shortens by a few days, or that your period arrives slightly earlier than expected. These changes reflect declining inhibin B and early fluctuations in follicle-stimulating hormone (FSH) [2]. Many women at this stage do not recognize these shifts as perimenopausal.
Mid Perimenopause
As the transition progresses, cycle irregularity becomes more pronounced. Periods may arrive weeks apart, or you may skip a month entirely. Anovulatory cycles, where the ovary does not release an egg, become more frequent. These cycles can produce heavier-than-usual bleeding because estrogen continues to stimulate the uterine lining without the balancing effect of progesterone from ovulation [3]. Heavy or prolonged bleeding during this phase warrants evaluation to rule out structural causes such as polyps or fibroids.
Late Perimenopause
In late perimenopause, gaps between periods lengthen to 60 days or more. Bleeding may become lighter and less frequent, or some women experience unpredictable episodes of heavy bleeding. The final menstrual period is identified only in retrospect, after 12 consecutive months without menstruation [2].
Menstrual cycle changes in perimenopause
2. Sleep and Circadian Rhythm
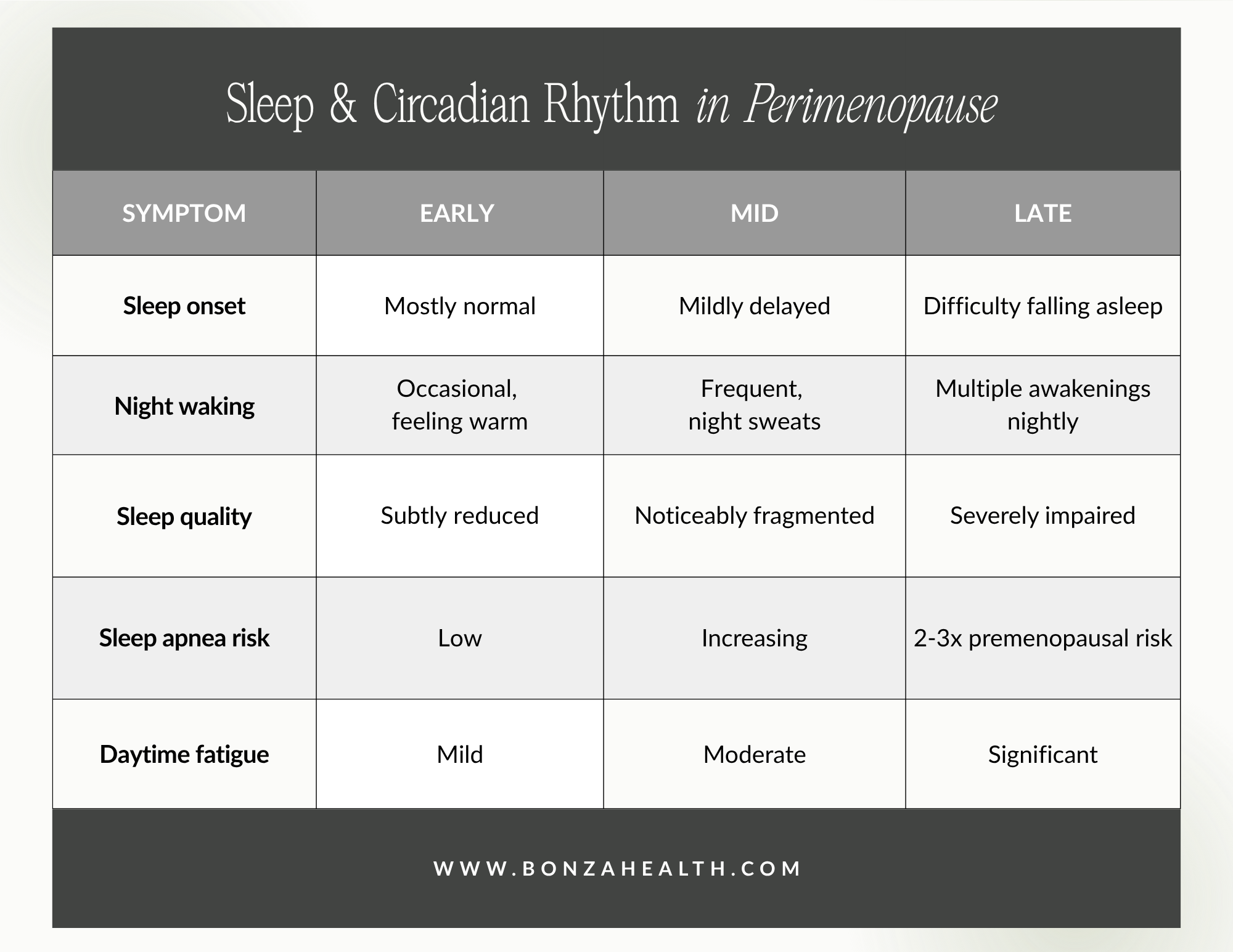
Sleep disturbances are among the most impactful symptoms of perimenopause, affecting up to 42% of women in the early transition and worsening as the transition progresses [4]. Poor sleep cascades into daytime fatigue, impaired cognitive function, mood changes, and reduced quality of life.
Early Perimenopause
Sleep disruption in early perimenopause is often subtle. Women may report feeling too warm at night, even before classic hot flashes appear. Research from the SWAN study found that women in early perimenopause reported shorter sleep duration and poorer sleep quality compared to premenopausal women of the same age [5]. Nocturia, or waking to urinate, may also begin to emerge as an early disruptor.
Mid Perimenopause
As hormone fluctuations intensify, night sweats become a more common cause of nighttime awakenings. Sleep fragmentation increases, and difficulty returning to sleep after waking becomes a hallmark complaint. The interplay between vasomotor symptoms, rising anxiety, and hormonal shifts creates a cycle that erodes sleep quality progressively [4]. Approximately 26% of perimenopausal women meet diagnostic criteria for chronic insomnia at this stage [6].
Late Perimenopause
In late perimenopause, sleep disturbances reach their peak. Women in the late perimenopausal stage have 1.3 times the adjusted odds of poor sleep quality compared to those in early perimenopause [7]. Night sweats may occur multiple times per night, and the resulting sleep deprivation contributes to cognitive difficulties and mood instability. Sleep-disordered breathing, including obstructive sleep apnea, also becomes more prevalent as the protective effects of estrogen and progesterone on upper airway tone diminish [4].
Sleep and circadian rhythm in perimenopause
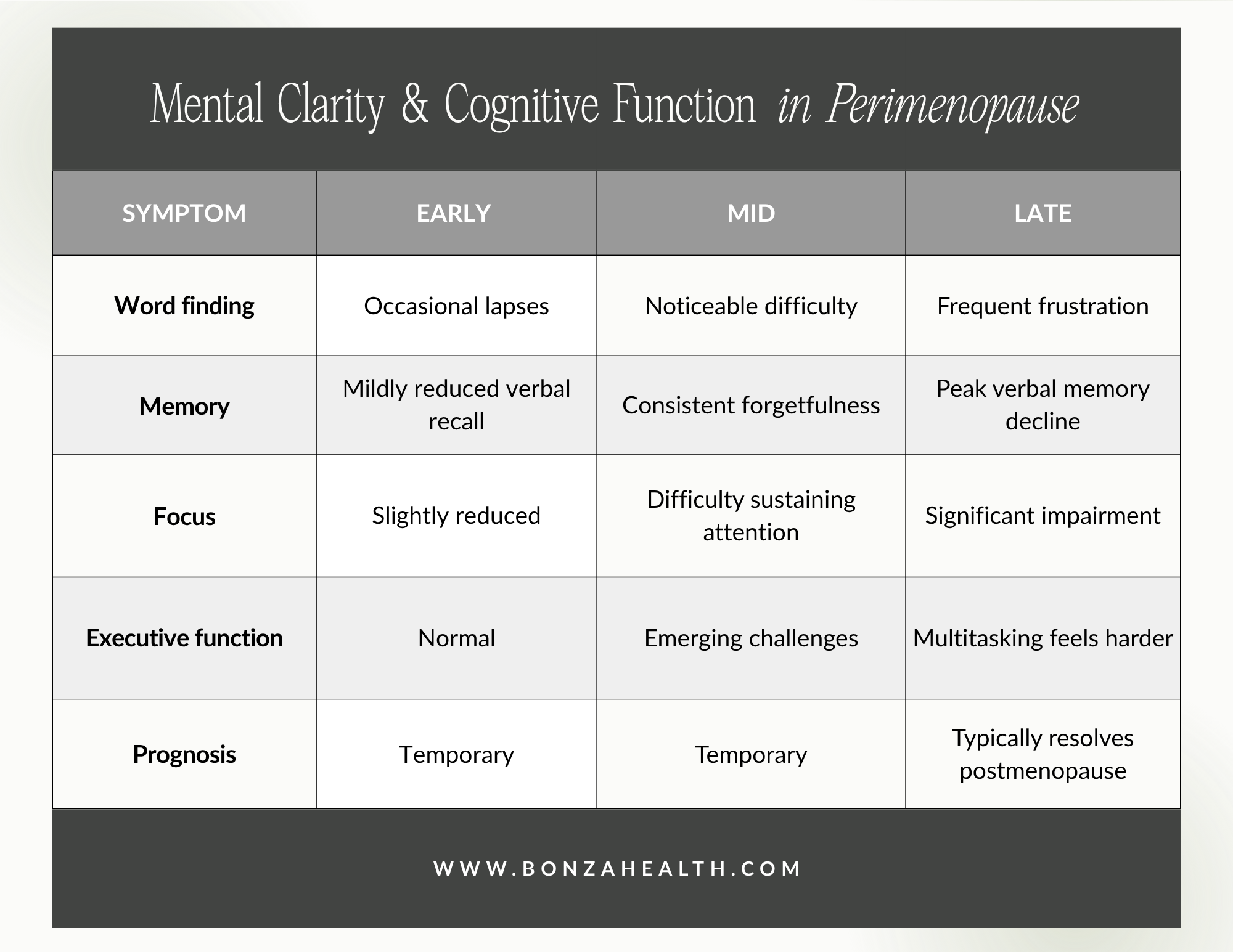
3. Mental Clarity and Cognitive Function
Brain fog is one of the most distressing and commonly reported symptoms of perimenopause. Women describe difficulty finding words, problems with concentration, forgetfulness, and a general sense that their mental sharpness has dulled. These experiences are real, measurable, and directly linked to hormonal changes [8].
Early Perimenopause
Cognitive changes in early perimenopause tend to be mild and episodic. You might notice occasional difficulty recalling names or an increased need to write things down. Research from the SWAN study demonstrated that verbal memory, specifically the ability to learn and recall new information, begins to decline during the early transition [8]. These changes often go unrecognized or are attributed to stress and aging.
Mid Perimenopause
As the transition deepens, cognitive complaints become more consistent. Difficulties with executive function, including planning, multitasking, and processing speed, may emerge. Studies show that perimenopausal women with worse sleep quality and more vasomotor symptoms tend to exhibit more pronounced cognitive difficulties [8]. The interaction between poor sleep, hot flashes, and depressed mood creates a compounding effect on mental clarity.
Late Perimenopause
Cognitive difficulties typically peak during late perimenopause. Verbal learning and memory weaknesses during this phase have been associated with greater depressive symptoms, more sleep disturbance, and worse vasomotor symptoms [8]. The encouraging news is that longitudinal research suggests these cognitive changes are largely temporary. Most women experience a return to baseline cognitive function in the postmenopausal period, once hormone levels stabilize [8].
Mental clarity and cognitive function in perimenopause
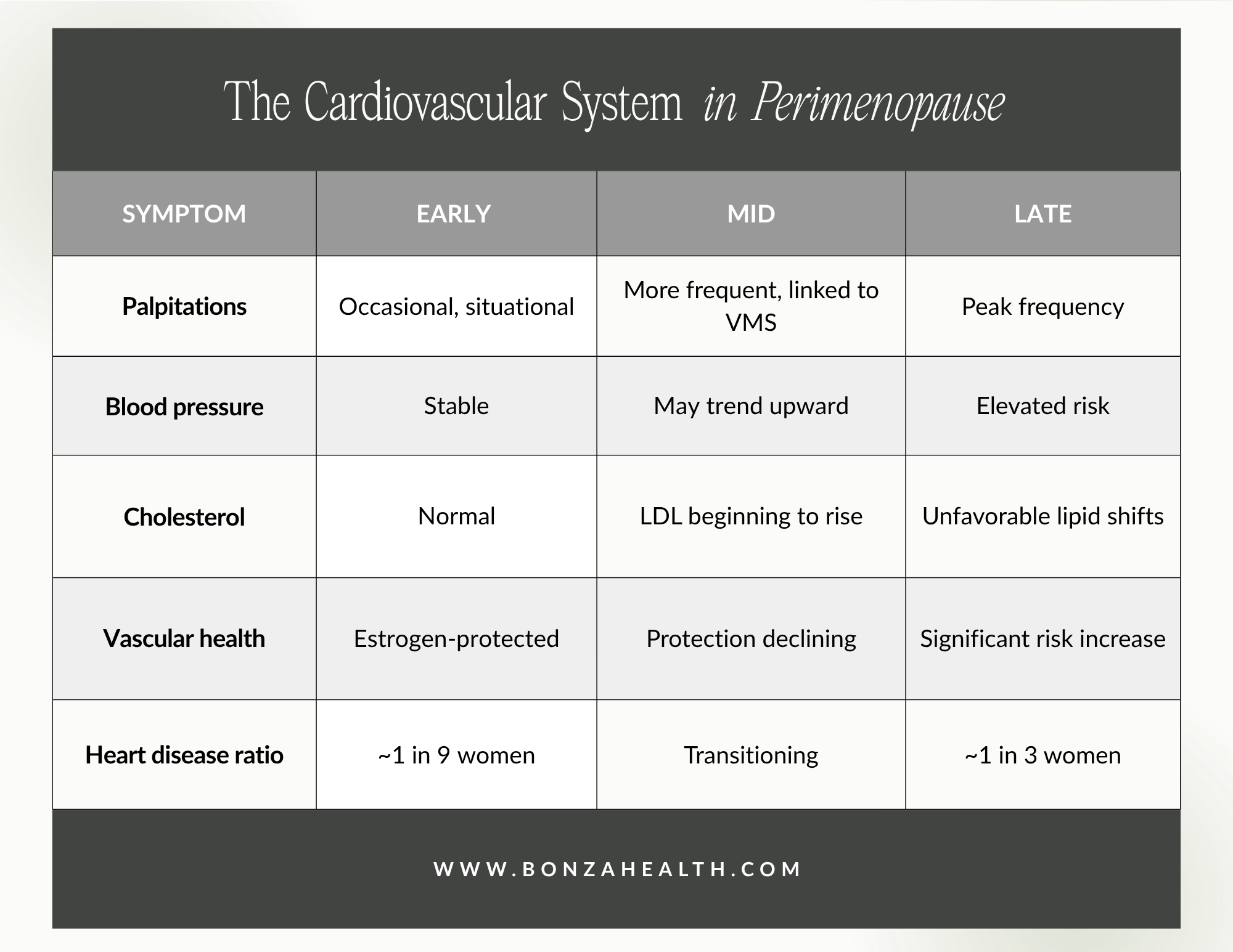
4. Cardiovascular System
Many women are surprised to learn that perimenopause affects the heart. Palpitations, the sensation of a racing, pounding, or skipping heartbeat, are reported by up to 42% of perimenopausal women [9]. Beyond palpitations, the cardiovascular risk profile shifts significantly as estrogen levels decline.
Early Perimenopause
In early perimenopause, cardiovascular symptoms are often subtle. Occasional palpitations may occur, frequently in association with anxiety or stress. Estrogen, which plays a protective role in vascular health by promoting vasodilation and favorable cholesterol profiles, begins to fluctuate, but its protective effects remain largely intact. Heart rate may transiently increase during early vasomotor episodes [10].
Mid Perimenopause
As estrogen fluctuations become more dramatic, palpitations may increase in frequency and intensity. Data from the SWAN study identified that approximately 16% of women fall into a high-probability palpitations trajectory during perimenopause, and an additional 34% experience moderate palpitations [11]. Palpitations during this phase are independently associated with vasomotor symptoms and anxiety [12]. Blood pressure and cholesterol levels may begin to trend upward.
Late Perimenopause
The late perimenopausal phase marks a critical inflection point for cardiovascular health. The ratio of women with heart disease jumps from approximately one in nine before menopause to one in three after menopause [10]. Low-density lipoprotein (LDL) cholesterol rises, high-density lipoprotein (HDL) cholesterol may decrease, and arterial stiffness increases. Palpitations often peak during this phase and into early postmenopause before gradually diminishing [11]. Any new-onset palpitations accompanied by chest pain, shortness of breath, or fainting warrant prompt medical evaluation.
The cardiovascular system in perimenopause
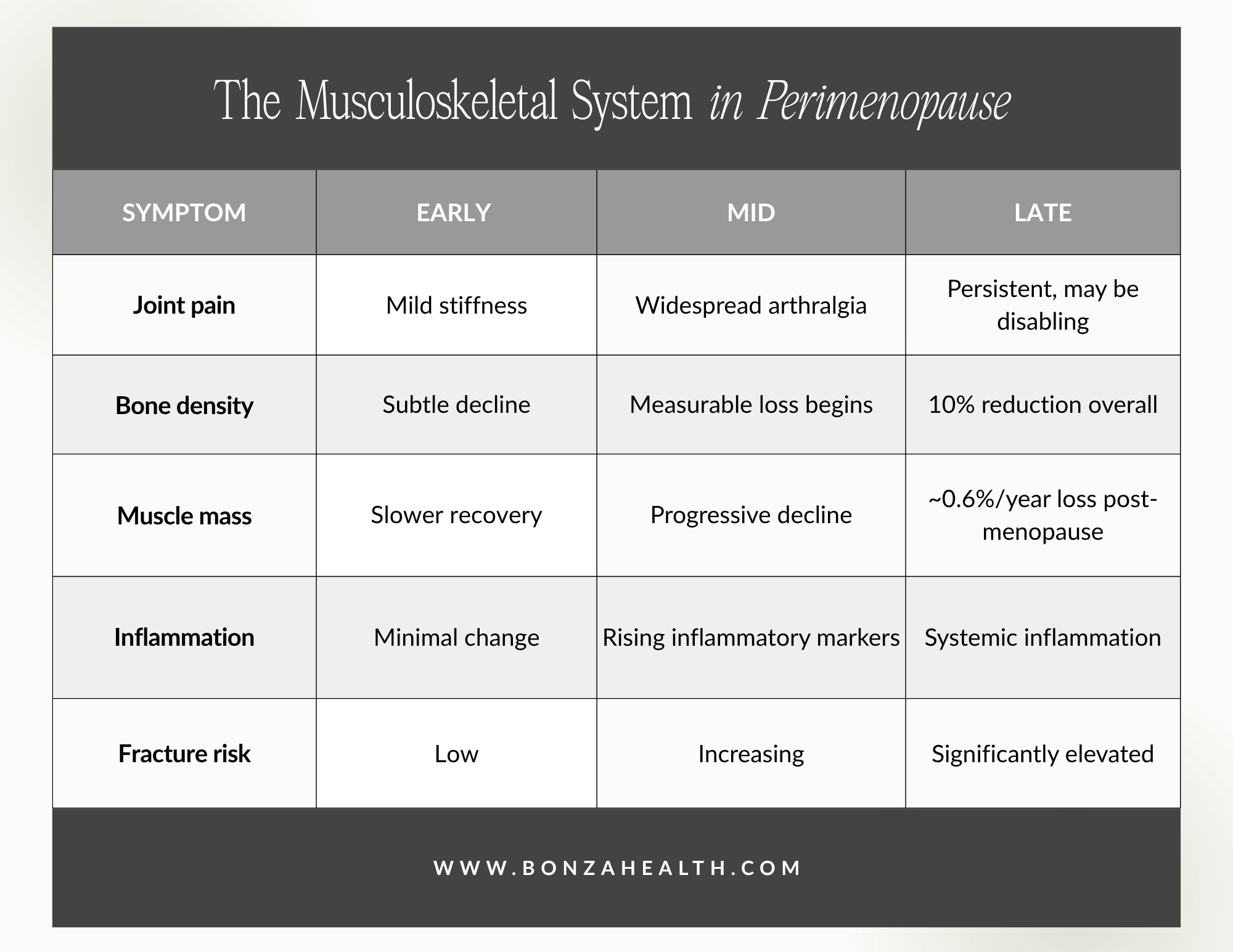
5. Musculoskeletal System
Musculoskeletal symptoms during perimenopause are remarkably common yet frequently overlooked. Approximately 70% of perimenopausal women report some form of musculoskeletal complaint, including joint pain, stiffness, loss of muscle mass, and decreased bone density [13]. Estrogen receptors are present in bone, cartilage, synovial membranes, muscles, and tendons, which explains why the decline in estrogen has such widespread musculoskeletal consequences [14].
Early Perimenopause
Joint stiffness and vague musculoskeletal aches may appear in early perimenopause, often dismissed as the natural consequence of aging or overuse. Bone mineral density begins to decline subtly during this phase, though the changes are not yet clinically significant in most women [15]. Muscle recovery after exercise may take longer than before, and women may notice that they lose strength more easily without consistent training.
Mid Perimenopause
Musculoskeletal pain becomes more prevalent and bothersome during mid-perimenopause. Perimenopausal women have a 63% higher risk of musculoskeletal pain compared to premenopausal women [16]. Conditions such as adhesive capsulitis (frozen shoulder) and tendinopathies peak in incidence during this phase. The decline in estrogen triggers increased systemic inflammation, which contributes to generalized arthralgia even in the absence of structural joint damage [14].
Late Perimenopause
In late perimenopause, bone loss accelerates significantly. Women experience an average reduction of 10% in bone mineral density during the perimenopausal transition, with the most rapid loss occurring in the two years before and three years after the final menstrual period [15]. Muscle mass declines at a rate of approximately 0.6% per year after menopause, a process known as sarcopenia [15]. Musculoskeletal syndrome of menopause, a recently proposed clinical term, describes the collective impact of arthralgia, bone loss, muscle loss, and osteoarthritis progression during this period [14].
The musculoskeletal system in perimenopause
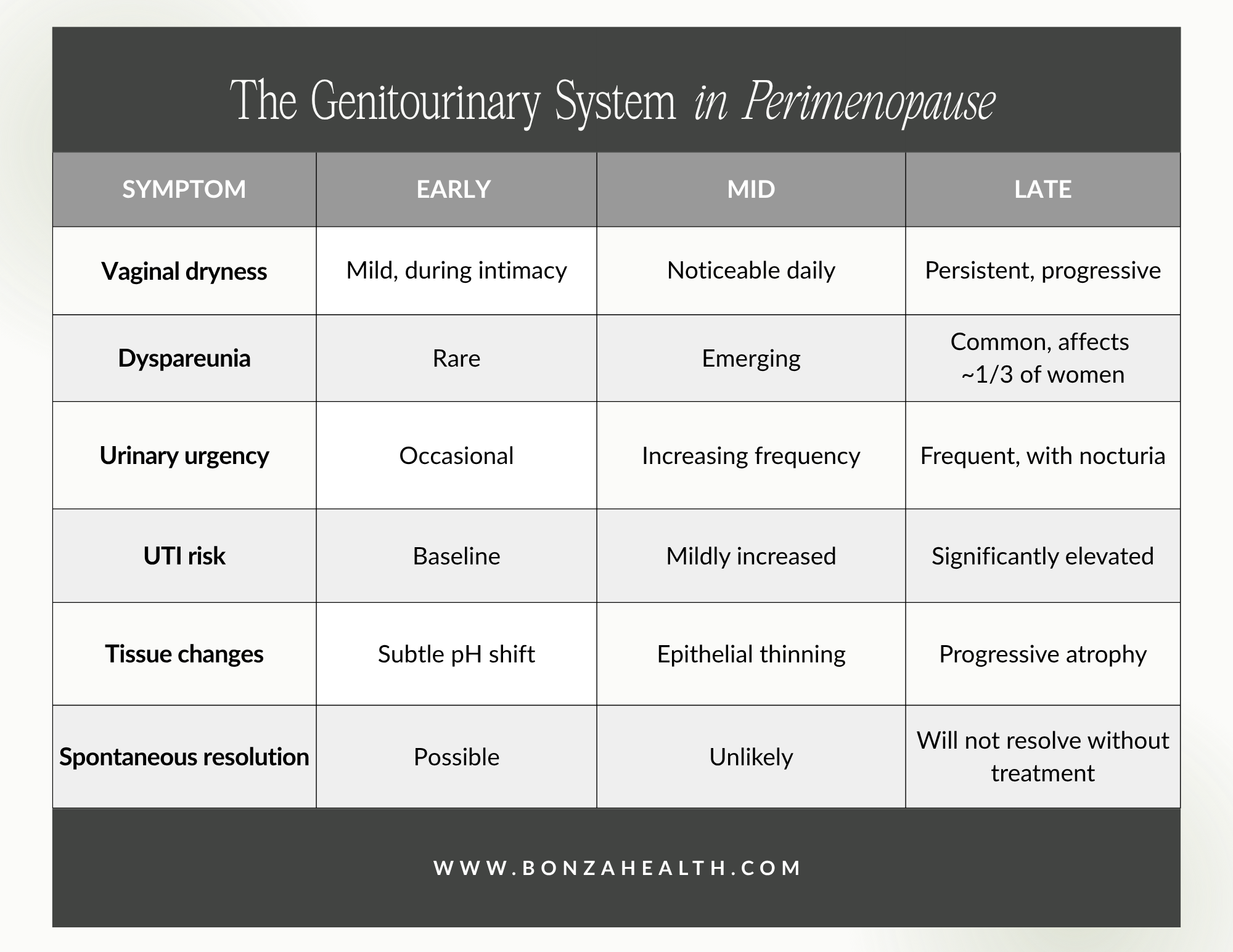
6. Genitourinary System
The genitourinary syndrome of menopause (GSM) is a chronic, progressive condition affecting the vulva, vagina, and lower urinary tract. Unlike vasomotor symptoms, which often improve after the transition, GSM symptoms tend to worsen over time without treatment [17]. Approximately 15% of premenopausal women experience early features of GSM, rising to 40-54% in postmenopausal women [18].
Early Perimenopause
In early perimenopause, genitourinary changes are subtle. You might notice a slight decrease in vaginal lubrication during intimacy, or mild urinary urgency that was not present before. Vaginal pH begins to shift as estrogen levels fluctuate, and the vaginal microbiome may start to change. These early signs are often attributed to dehydration, stress, or urinary tract infections rather than recognized as hormonal in origin.
Mid Perimenopause
As estrogen levels decline more consistently, vaginal dryness becomes noticeable outside of sexual activity. The vaginal epithelium begins to thin, and women may experience irritation, burning, or discomfort with daily activities such as sitting or walking. Urinary symptoms including increased frequency, urgency, and recurrent urinary tract infections may emerge. Dyspareunia, or painful intercourse, begins to affect intimate relationships [17].
Late Perimenopause
Late perimenopause marks the beginning of progressive, often permanent, genitourinary tissue changes unless treatment is initiated. Vaginal dryness affects approximately one-third of women in this phase, and unlike hot flashes and mood symptoms, these changes will not resolve spontaneously [3]. Vulvar atrophy can make sitting, exercising, and urination uncomfortable. The risk of recurrent urinary tract infections increases as the vaginal microbiome shifts and protective lactobacilli decline. This is the phase where proactive treatment, whether with vaginal moisturizers, topical estrogen, or other therapies, can make the most meaningful difference in quality of life.
The genitourinary system in perimenopause
When to Talk to Your Doctor
If you are in your late thirties or forties and are experiencing any combination of the symptoms described above, it may be time to have a conversation with a healthcare provider who understands the menopause transition. You do not need to wait until your periods have stopped or until symptoms become unbearable. Early recognition leads to earlier intervention, and earlier intervention leads to better outcomes.
Symptoms that warrant prompt evaluation include new-onset palpitations with chest pain or shortness of breath, heavy or prolonged menstrual bleeding, significant mood changes or suicidal thoughts, urinary symptoms suggestive of infection, and any rapid change in symptom severity.
For the many symptoms of perimenopause that are uncomfortable but not dangerous, a range of evidence-based treatments exists, from lifestyle modifications and behavioral therapies to hormone therapy and targeted medications. You deserve to feel supported through this transition, and you deserve a provider who will listen.

At Bonza Health, we specialize in guiding women through every phase of the menopause transition. If any of this sounds familiar, we are here to help. Visit us at www.bonzahealth.com to schedule your consultation.
References
[1] N. Santoro, "Perimenopause: From Research to Practice," J. Clin. Endocrinol. Metab., vol. 101, no. 9, pp. 3594-3602, 2016, doi: 10.1210/jc.2015-4012. [PubMed: 26653408]
[2] S. D. Harlow et al., "Executive summary of the Stages of Reproductive Aging Workshop +10," J. Clin. Endocrinol. Metab., vol. 97, no. 4, pp. 1159-1168, 2012, doi: 10.1210/jc.2011-3362. [PMC: PMC3319184]
[3] L. Delamater and N. Santoro, "Management of the Perimenopause," Clin. Obstet. Gynecol., vol. 61, no. 3, pp. 419-432, 2018, doi: 10.1097/GRF.0000000000000389. [PubMed: 29952797]
[4] A. Preti et al., "Sleep Disturbance and Perimenopause: A Narrative Review," J. Clin. Med., vol. 14, no. 5, p. 1479, 2025, doi: 10.3390/jcm14051479. [PubMed: 40094961]
[5] H. J. Jones, R. Zak, and K. A. Lee, "Sleep Disturbances in Midlife Women at the Cusp of the Menopausal Transition," J. Clin. Sleep Med., vol. 14, no. 7, pp. 1127-1133, 2018, doi: 10.5664/jcsm.7208.
[6] J. Lampio et al., "Insomnia in midlife: a longitudinal study," Sleep, vol. 40, no. 10, 2017, doi: 10.1093/sleep/zsx135.
[7] A. A. Bruyneel, "Longitudinal Study of Insomnia Symptoms Among Women During Perimenopause," J. Obstet. Gynecol. Neonatal Nurs., vol. 46, no. 6, pp. 804-813, 2017, doi: 10.1016/j.jogn.2017.07.011. [PMC: PMC5776689]
[8] C. A. Metcalf et al., "Cognitive Problems in Perimenopause: A Review of Recent Evidence," Curr. Psychiatry Rep., vol. 25, no. 10, pp. 501-511, 2023, doi: 10.1007/s11920-023-01447-3. [PMC: PMC10842974]
[9] J. S. Carpenter et al., "Correlates of palpitations during menopause: A scoping review," Women's Health, vol. 18, 2022, doi: 10.1177/17455057221112267. [PMC: PMC9289918]
[10] C. N. Bairey Merz et al., "Cardiovascular disease in women: A statement from the American Heart Association," Circulation, vol. 144, pp. e107-e130, 2021.
[11] J. S. Carpenter et al., "Palpitations across the menopause transition in SWAN," Menopause, vol. 30, no. 1, pp. 25-35, 2023, doi: 10.1097/GME.0000000000002083. [PMC: PMC9797427]
[12] M. Terauchi et al., "Independent association of palpitation with vasomotor symptoms and anxiety in middle-aged women," Menopause, vol. 28, no. 10, pp. 1143-1150, 2021, doi: 10.1097/GME.0000000000001808. [PubMed: 34033601]
[13] V. J. Wright et al., "The musculoskeletal syndrome of menopause," Climacteric, vol. 27, no. 5, pp. 466-472, 2024, doi: 10.1080/13697137.2024.2380363. [PubMed: 39077777]
[14] R. M. J. Palmer et al., "Joint pain and menopause," Menopause, 2025. [PMC: PMC12915535]
[15] X. Lu et al., "Musculoskeletal Pain during the Menopausal Transition: A Systematic Review and Meta-Analysis," Int. J. Environ. Res. Public Health, vol. 17, no. 21, p. 7760, 2020, doi: 10.3390/ijerph17217760. [PMC: PMC7710408]
[16] F. E. Watt, "Musculoskeletal pain and menopause," Post Reprod. Health, vol. 24, no. 1, pp. 34-43, 2018, doi: 10.1177/2053369118757537. [PubMed: 29412042]
[17] K. Angelou et al., "The Genitourinary Syndrome of Menopause: An Overview of the Recent Data," Cureus, vol. 12, no. 4, p. e7586, 2020, doi: 10.7759/cureus.7586. [PMC: PMC7212735]
[18] J. Gandhi et al., "Genitourinary syndrome of menopause: an overview," Am. J. Obstet. Gynecol., vol. 215, no. 6, pp. 704-711, 2016, doi: 10.1016/j.ajog.2016.07.045. [PubMed: 27472999]