
Building Bones for Life: A Perimenopausal Woman's Guide to Preventing Osteoporosis
Written and edited by Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

By the time many women notice their first hot flash or skipped period, their bones have already started a quiet countdown. In the years surrounding menopause, women can lose up to 10% of their bone mass — and the steepest decline begins in perimenopause, often before any "official" diagnosis of menopause is made. The good news? This is also when intervention works best. Bone is living tissue. It responds — sometimes dramatically — to mechanical loading, hormonal signaling, and the right micronutrients.
This guide covers the four pillars of perimenopausal bone protection: strategic exercise, whole-body vibration, early estradiol therapy, and targeted nutrient support (vitamin D3 with K2) — all backed by peer-reviewed evidence.
Why Perimenopause Is the Critical Window
Estrogen is one of the most powerful regulators of bone remodeling. It restrains osteoclasts (the cells that break bone down) and supports osteoblasts (the cells that build it up). As estradiol levels begin to fluctuate and decline in perimenopause, bone resorption outpaces bone formation. The result is accelerated bone loss that can continue for 5–10 years.
The concept of the "window of opportunity" — initiating menopausal hormone therapy within 10 years of menopause or before age 60 — has become central to modern menopause medicine because the benefits to bone (and the cardiovascular and overall safety profile) are most favorable during this period.

Weight-bearing exercise is crucial for bone health
Pillar 1: Move With Purpose—The Right Kind of Exercise
Not all exercise is created equal when it comes to bone. The skeleton responds to mechanical strain: high-magnitude, high-rate forces applied at unusual angles. Walking is wonderful for the heart and mood, but it loads the skeleton at only about 1.0–1.2 times body weight. Jumping can deliver 3–6 times body weight. That difference is everything.
High-Impact Exercise: The Gold Standard
A 2023 systematic review concluded that high-intensity and high-impact exercises are the most effective non-pharmacological tools to maintain or improve bone mineral density (BMD) in the lumbar spine and femoral neck of postmenopausal women (Pinheiro MB et al., 2023; Senderovich H et al., Cureus, PMC9990535).
The classic Heinonen et al. trial randomized 98 premenopausal women aged 35–45 to 18 months of progressive high-impact training (jumps from 10–25 cm boxes generating 2.1–5.6× body weight forces). The exercise group showed significant gains in femoral neck BMD compared to controls (Heinonen A et al., Lancet 1996;348:1343–1347).
The LIFTMOR trial changed the conversation about whether older women with low bone mass could safely train at high intensity. Watson and colleagues randomized 101 postmenopausal women with osteopenia or osteoporosis to either eight months of high-intensity resistance and impact training (HiRIT) — including deadlifts, overhead press, back squats, and jumping chin-ups with drop landings — or a low-intensity home program. The HiRIT group significantly improved lumbar spine BMD, femoral neck BMD, and physical function, with excellent safety (Watson SL et al., J Bone Miner Res 2018;33(2):211–220).

Running generates ground reaction forces of approximately 2.5–3× body weight; jumping rope produces similar forces with the added benefit of being repetitive, rhythmic, and easily progressed.
Jumping: Cheap, Fast, and Effective
Jumping protocols are remarkably efficient. Sugiyama and colleagues found that just 10–20 jumps performed twice daily for 16 weeks significantly increased hip BMD in premenopausal women aged 25–50 (Sugiyama T et al., Am J Health Promot 2014; PMID 24460005). Kato et al. demonstrated that 10 maximum vertical jumps three times per week for six months significantly increased femoral neck BMD in young women (Kato T et al., J Appl Physiol 2006).
Running and Jumping Rope
Running generates ground reaction forces of approximately 2.5–3× body weight; jumping rope produces similar forces with the added benefit of being repetitive, rhythmic, and easily progressed. Both stimulate osteogenic adaptation at the hip and spine — the two most fracture-prone sites.
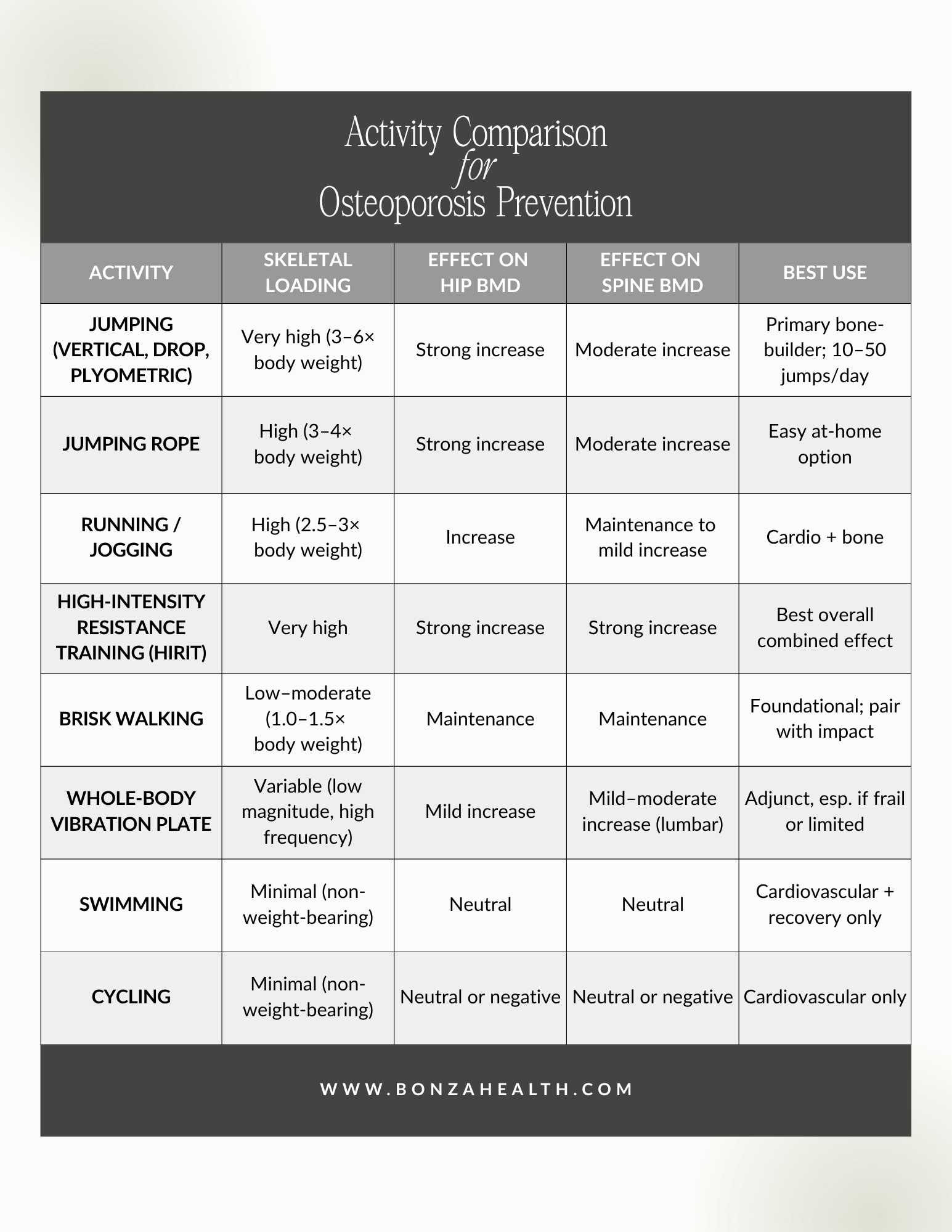
Activity Comparison for Osteoporosis Prevention
Walking: Necessary But Not Sufficient
Walking helps preserve what you have but rarely builds new bone in adults. Cross-sectional studies show that habitual walking is associated with modestly higher hip BMD, but randomized trials of walking alone in postmenopausal women generally show maintenance — not gain — of BMD. Walking is foundational, but it works best when paired with impact and resistance training.
Swimming: A Mixed Bag
Swimming is fantastic for cardiovascular health, joint comfort, and mood, but as a non-weight-bearing activity it produces minimal mechanical loading on the skeleton. A 2020 meta-analysis of five randomized trials (263 participants) found that swimming did not significantly improve BMD at the spine or femoral neck in pre- or postmenopausal women, though it may help maintain bone in older swimmers (Su Y et al., BioMed Res Int 2020;2020:6210201). Swimming should complement — not replace — weight-bearing and impact work for bone health.
Resistance Training
Heavy progressive resistance training (loads at 80–85% of one-rep maximum) reliably improves BMD when performed 2–3 times per week. Compound lifts (squats, deadlifts, presses) are particularly effective because they load the spine and hips directly.
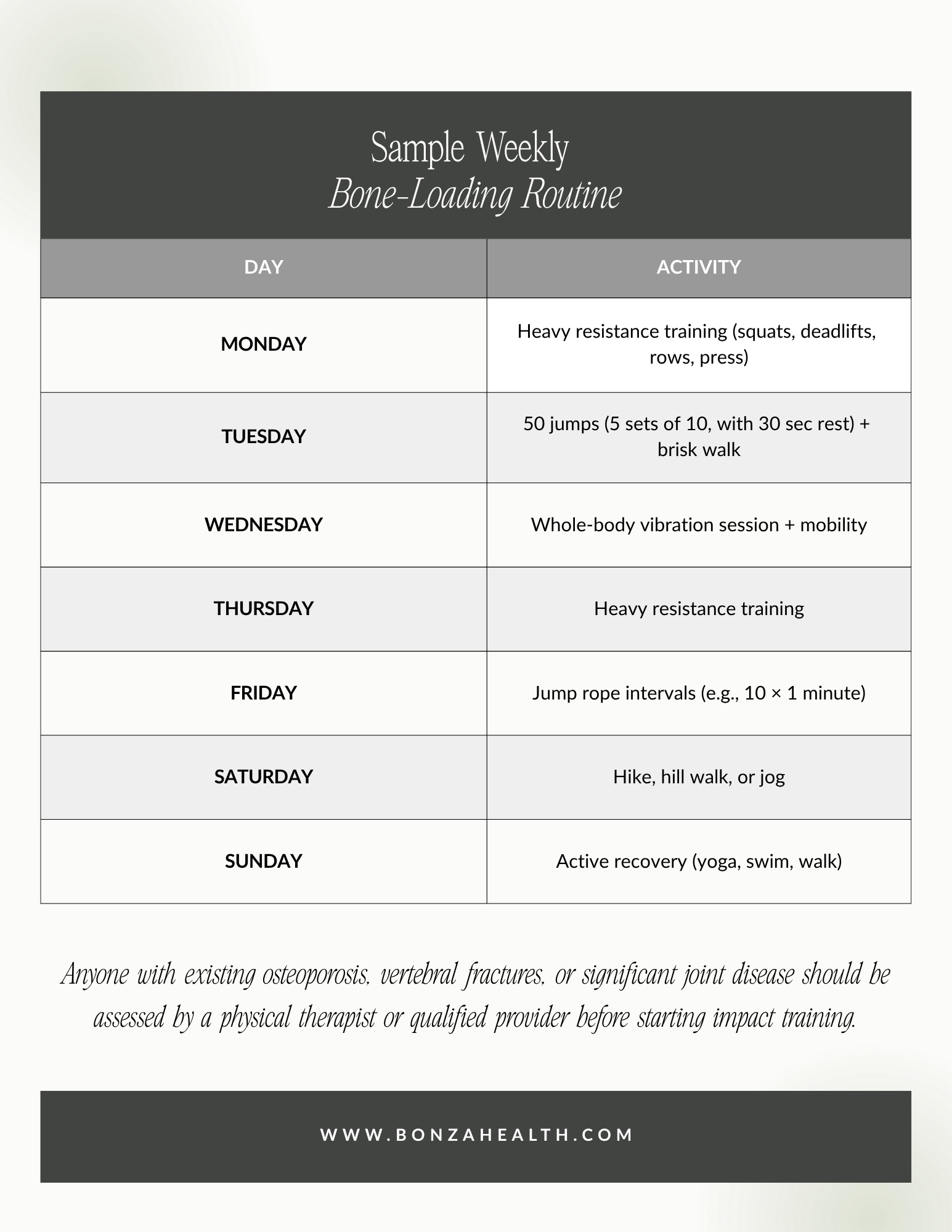
Sample Weekly Bone-Loading Routine
Pillar 2: Whole-Body Vibration—The Underrated Adjunct
A vibration plate is exactly what it sounds like: a platform that delivers controlled mechanical oscillations through the feet into the muscles and bones. The proposed mechanism involves activation of mechanosensitive ion channels (Piezo1/2) in osteocytes, triggering anabolic signaling pathways including Wnt/β-catenin.
A 2023 systematic review and meta-analysis of 23 studies concluded that whole-body vibration (WBV) using high frequency (~30 Hz), low magnitude (~0.3 g), and high cumulative dose (~7,000 minutes) significantly improved lumbar spine BMD in postmenopausal women, with high-quality (GRADE) evidence (de Oliveira RDJ et al., Osteoporos Int 2023;34(1):29–52; PMID 36282343).
A 2018 meta-analysis by Marín-Cascales and colleagues likewise showed a significant pre-to-post improvement in lumbar spine BMD with WBV training (Marín-Cascales E et al., Medicine (Baltimore) 2018;97(34):e11918; PMID 30142802). The original Rubin et al. trial showed that low-magnitude, high-frequency mechanical signals could prevent postmenopausal bone loss in a clinical population (Rubin C et al., J Bone Miner Res 2004;19:343–351).
Vibration is particularly appealing for women who cannot perform impact exercise due to joint limitations, balance concerns, or deconditioning. It does not replace resistance and impact training in robust women — but it is a meaningful add-on.
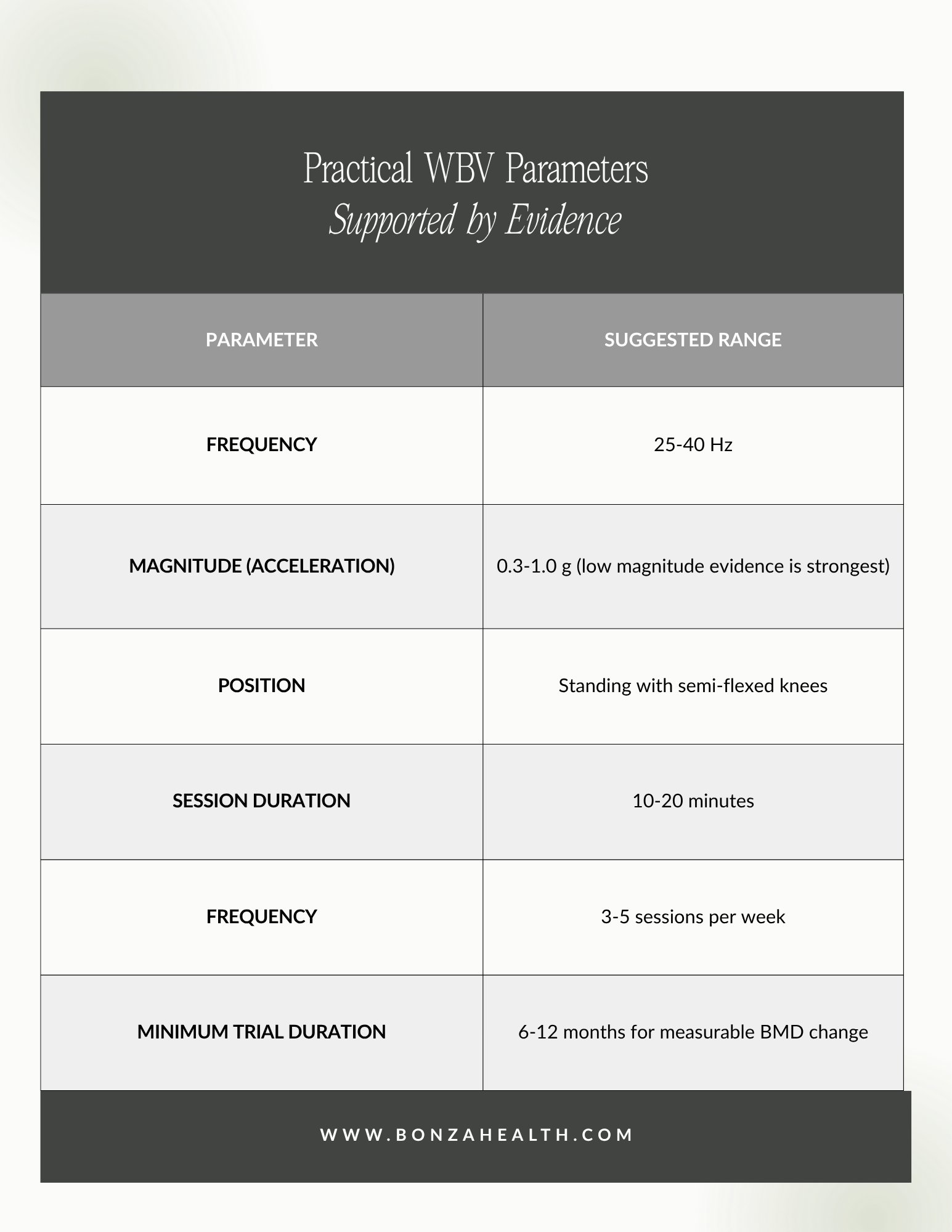
Practical WBV Parameters Supported by Evidence
Pillar 3: Early Estradiol Therapy—Treating the Root Cause
If estrogen loss drives perimenopausal bone loss, then replacing estradiol logically prevents it. Decades of evidence confirm this.
The Women's Health Initiative — despite the controversies in its initial interpretation — demonstrated a 33% reduction in hip fractures among women on combined hormone therapy versus placebo, with fracture benefit persisting 13 years later (Levin VA et al., Climacteric/Osteoporos Int review, PMID 29520604).
Even ultralow-dose 17β-estradiol (0.25 mg/day) has been shown to increase total body and hip BMD over three years in older postmenopausal women, with minimal endometrial stimulation (Prestwood KM et al., JAMA 2003;290:1042–1048).
A systematic review of menopausal hormone therapy and bone confirms that timing matters: the bone-protective benefits of estradiol are greatest when therapy is initiated during perimenopause or within the first 10 years of menopause — the so-called "window of opportunity" (Frontiers in Reproductive Health 2025 scoping review; doi:10.3389/frph.2025.1542746). Long-term, low-dose regimens preserve BMD for years; high doses are not required.
Forms of estradiol used for bone protection include:
Transdermal patches (e.g., 0.025–0.1 mg/day) — preferred for cardiovascular and clotting safety
Topical gels and sprays with verified absorption
Oral estradiol (1–2 mg/day) when transdermal is not feasible
Women with an intact uterus require concurrent progestogen (typically micronized progesterone) for endometrial protection.
Importantly, recent data suggest that estradiol blood levels achieved on therapy vary widely between women on the same dose. Glynne and colleagues found that approximately 1 in 4 women on the highest licensed dose of transdermal estrogen had subtherapeutic estradiol levels (Glynne S et al., Menopause 2025). Verifying levels through serum or dried-urine testing helps ensure that the dose is high enough to actually protect bone — not just relieve hot flashes.
What Counts as an "Adequate" Bone-Protective Estradiol Level?
Most experts target serum estradiol levels of approximately 40–60 pg/mL for bone protection, though optimal individualized targets should be discussed with a knowledgeable clinician.

If estrogen loss drives perimenopausal bone loss, then replacing estradiol logically prevents it.
Pillar 4: Vitamin D3 and K2—The Bone-Mineralizing Duo
Calcium gets all the press, but two fat-soluble vitamins govern where calcium ultimately ends up: in bone, where you want it, or in arteries and soft tissue, where you don't.
Vitamin D3 (cholecalciferol) is essential for intestinal calcium absorption and supports the differentiation of osteoblasts. Low 25(OH) vitamin D levels are associated with secondary hyperparathyroidism, increased bone turnover, and accelerated bone loss. Most experts target a 25(OH)D level of 40–60 ng/mL for skeletal and overall health.
Vitamin K2 (especially as menaquinone-7, MK-7) activates osteocalcin — the protein that binds calcium into the bone matrix — through γ-carboxylation. K2 also activates matrix Gla protein, which prevents calcium from depositing in arterial walls.
The landmark 3-year randomized trial by Knapen and colleagues followed 244 healthy postmenopausal women receiving either placebo or 180 μg/day of MK-7. The MK-7 group showed:
Significantly improved vitamin K status (decreased uncarboxylated osteocalcin)
Decreased age-related decline in BMD at the lumbar spine and femoral neck
Improved bone strength indices at the femoral neck
Reduced loss of vertebral height
(Knapen MHJ et al., Osteoporos Int 2013;24(9):2499–2507; PMID 23525894)
Earlier work by Ushiroyama and colleagues showed that 24 months of combined K2 + D3 therapy increased BMD by approximately 4.9%, while K2 alone produced negligible change — a strong argument for using these nutrients together (Ushiroyama T et al., Maturitas 2002;41:211–221).
Not all studies are positive; a 3-year trial of high-dose MK-7 (375 μg) in osteopenic women on calcium and D3 found no additional BMD benefit but did improve vitamin K status (Rønn SH et al., Osteoporos Int 2021; PMID 33030563). Heterogeneity in dose, baseline vitamin status, and study population likely explains discrepancies.
The MOTS trial (combined melatonin, strontium citrate, vitamin D3, and K2) showed a 4.3% BMD increase at the lumbar spine and 2.2% at the femoral neck in osteopenic postmenopausal women over 1 year (Maria S et al., J Orthop Translat 2017; PMID 28130552).
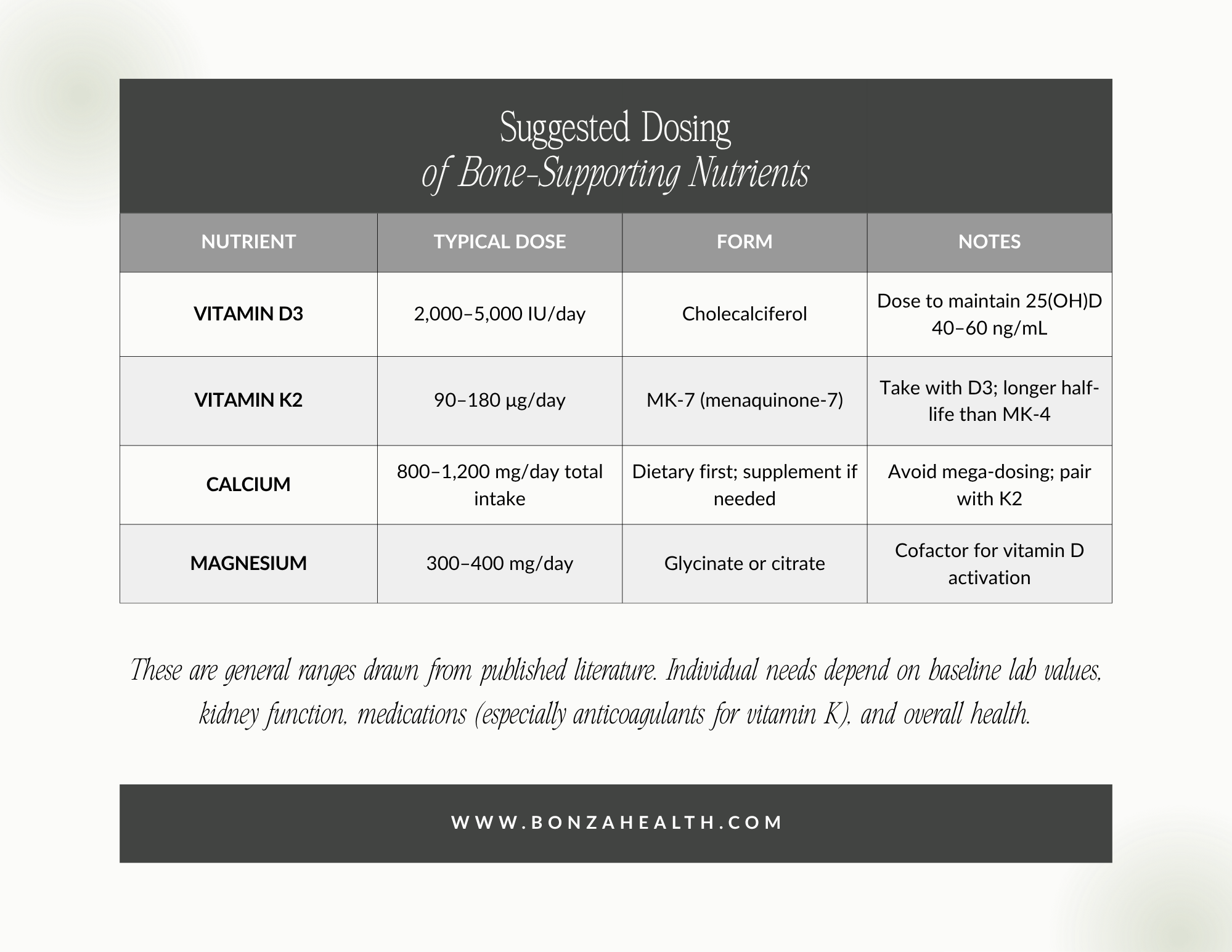
Suggested Dosing of Bone-Supporting Nutrients
Putting It Together: A Practical Framework
A bone-protective perimenopausal protocol typically integrates all four pillars:
Move smart: 2–3 sessions of resistance training, daily impact (jumps, jump rope, or running), and brisk walking on most days. Add whole-body vibration 3–5×/week if available.
Address hormones early: Discuss menopausal hormone therapy with a knowledgeable clinician before you have measurable bone loss — not after.
Optimize key nutrients: Vitamin D3, vitamin K2 (MK-7), magnesium, and adequate dietary protein and calcium.
Track progress: Baseline DXA scan, periodic bone turnover markers (CTX, P1NP), and 25(OH) vitamin D and estradiol levels guide individualized care.
Take the Next Step
If you're ready to translate this evidence into an individualized plan, the supplements you choose matter. Quality, dosing, and verified ingredients are not equal across the supplement market.
Sign up for Fullscript to access pharmaceutical-grade vitamin D3, MK-7, and other practitioner-curated bone-support formulas — delivered to your door, with the transparency and quality control your bones deserve. Use the link below to create your free Fullscript account and view the bone health protocol designed for perimenopausal women.

Your future self — strong, upright, and fracture-free at 80 — starts with the choices you make today.
References
Pinheiro MB, Oliveira J, Bauman A, et al. The role of high-intensity and high-impact exercises in improving bone health in postmenopausal women: a systematic review. Cureus. 2023. PMC9990535.
Heinonen A, Kannus P, Sievänen H, et al. Randomised controlled trial of effect of high-impact exercise on selected risk factors for osteoporotic fractures. Lancet. 1996;348:1343–1347.
Watson SL, Weeks BK, Weis LJ, Harding AT, Horan SA, Beck BR. High-intensity resistance and impact training improves bone mineral density and physical function in postmenopausal women with osteopenia and osteoporosis: the LIFTMOR randomized controlled trial. J Bone Miner Res. 2018;33(2):211–220. PMID 28975661.
Sugiyama T, Yamaguchi A, Kawai S. Effects of two jumping programs on hip bone mineral density in premenopausal women. Am J Health Promot. 2014. PMID 24460005.
Kato T, Terashima T, Yamashita T, Hatanaka Y, Honda A, Umemura Y. Effect of low-repetition jump training on bone mineral density in young women. J Appl Physiol. 2006;100(3):839–843.
Vainionpää A, Korpelainen R, Vihriälä E, Jämsä T. Effect of impact exercise on bone metabolism. Osteoporos Int. 2006;17(3):411–422.
Su Y, Chen Z, Xie W. Swimming as treatment for osteoporosis: a systematic review and meta-analysis. BioMed Res Int. 2020;2020:6210201.
Abrahin O, Rodrigues RP, Marçal AC, et al. Swimming and cycling do not cause positive effects on bone mineral density: a systematic review. Rev Bras Reumatol. 2016;56(4):345–351.
de Oliveira RDJ, de Oliveira RG, de Oliveira LC, Santos-Filho SD, Sá-Caputo DC, Bernardo-Filho M. Effectiveness of whole-body vibration on bone mineral density in postmenopausal women: a systematic review and meta-analysis of randomized controlled trials. Osteoporos Int. 2023;34(1):29–52. PMID 36282343.
Marín-Cascales E, Alcaraz PE, Ramos-Campo DJ, Martinez-Rodriguez A, Chung LH, Rubio-Arias JÁ. Whole-body vibration training and bone health in postmenopausal women: a systematic review and meta-analysis. Medicine (Baltimore). 2018;97(34):e11918. PMID 30142802.
Rubin C, Recker R, Cullen D, Ryaby J, McCabe J, McLeod K. Prevention of postmenopausal bone loss by a low-magnitude, high-frequency mechanical stimuli: a clinical trial assessing compliance, efficacy, and safety. J Bone Miner Res. 2004;19:343–351.
Slatkovska L, Alibhai SM, Beyene J, Hu H, Demaras A, Cheung AM. Effect of 12 months of whole-body vibration therapy on bone density and structure in postmenopausal women: a randomized trial. Ann Intern Med. 2011;155(10):668–679.
Levin VA, Jiang X, Kagan R. Estrogen therapy for osteoporosis in the modern era. Osteoporos Int. 2018;29(5):1049–1055. PMID 29520604.
Prestwood KM, Kenny AM, Kleppinger A, Kulldorff M. Ultralow-dose micronized 17β-estradiol and bone density and bone metabolism in older women: a randomized controlled trial. JAMA. 2003;290(8):1042–1048.
Cauley JA, Robbins J, Chen Z, et al. Effects of estrogen plus progestin on risk of fracture and bone mineral density: the Women's Health Initiative randomized trial. JAMA. 2003;290(13):1729–1738.
Glynne S, Reisel D, Kamal A, et al. Suboptimal serum estradiol levels in women using transdermal hormone therapy: a real-world study. Menopause. 2025.
Knapen MHJ, Drummen NE, Smit E, Vermeer C, Theuwissen E. Three-year low-dose menaquinone-7 supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporos Int. 2013;24(9):2499–2507. PMID 23525894.
Ushiroyama T, Ikeda A, Ueki M. Effect of continuous combined therapy with vitamin K2 and vitamin D3 on bone mineral density and coagulofibrinolysis function in postmenopausal women. Maturitas. 2002;41(3):211–221.
Rønn SH, Harsløf T, Oei L, Pedersen SB, Langdahl BL. The effect of vitamin MK-7 on bone mineral density and microarchitecture in postmenopausal women with osteopenia: a 3-year randomized, placebo-controlled clinical trial. Osteoporos Int. 2021. PMID 33030563.
Maria S, Samsonraj RM, Munmun F, et al. Melatonin-micronutrients osteopenia treatment study (MOTS): a translational study assessing melatonin, strontium (citrate), vitamin D3 and vitamin K2 (MK7) on bone density. J Orthop Translat. 2017. PMID 28130552.
This article is for educational purposes and does not constitute medical advice. Decisions about hormone therapy, supplementation, and exercise should be made in partnership with a qualified clinician familiar with your individual health history.