
Is It ADHD, Perimenopause, or Both? What the Science Actually Says About the Diagnosis Surge in Midlife Women
Written and edited by Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Is it ADHD, perimenopause, or both?
If you've spent any time on social media in the past year, you've seen the wave: women in their 40s describing the same cluster of symptoms — losing words mid-sentence, missing deadlines for the first time in their lives, drowning in browser tabs and unfinished tasks — and asking the same question.
“Is this ADHD, or is this perimenopause?”
Mary Claire Haver's The New Menopause pulled the conversation into the mainstream, and a striking trend in the medical literature has caught up with it: women are being diagnosed with ADHD at unprecedented rates in midlife. One large 2024 analysis of hospital delivery records documented a 39.4% rise in ADHD diagnoses among women between 2016 and 2020.¹
So what's actually going on? And how do you sort out what's a hormone story, what's a neurodevelopmental story, and what — increasingly often — is both at once?
As a menopause-trained physician, here's how I think about it, drawing on traditional medicine, lifestyle medicine, and functional medicine.

If ADHD symptoms are significantly impairing your work, relationships, or quality of life, a formal evaluation is key.
The estrogen-dopamine connection: why perimenopause "feels like" ADHD
ADHD is fundamentally a dopamine and norepinephrine story. Estrogen is, too.
Estrogen enhances dopamine synthesis, slows its degradation, and amplifies its activity in the prefrontal cortex — the seat of executive function.² When estrogen begins to fluctuate (which can start in your late 30s, long before periods become irregular), dopaminergic signaling becomes erratic. The result: word-finding problems, distractibility, emotional dysregulation, and working memory lapses.
For women with undiagnosed ADHD, perimenopause is often when masking strategies finally collapse. The dopaminergic system was already running lean. Remove the estrogen scaffolding, and what was manageable becomes unmanageable. Systematic reviews consistently describe hormonal transitions as periods when ADHD symptoms intensify, and previously coping women seek diagnosis for the first time.³
This isn't either/or. Many midlife women genuinely have ADHD that was missed in childhood (girls were chronically underdiagnosed for decades) and are experiencing the cognitive impact of declining estrogen. Recognizing both pieces is what lets us actually help.
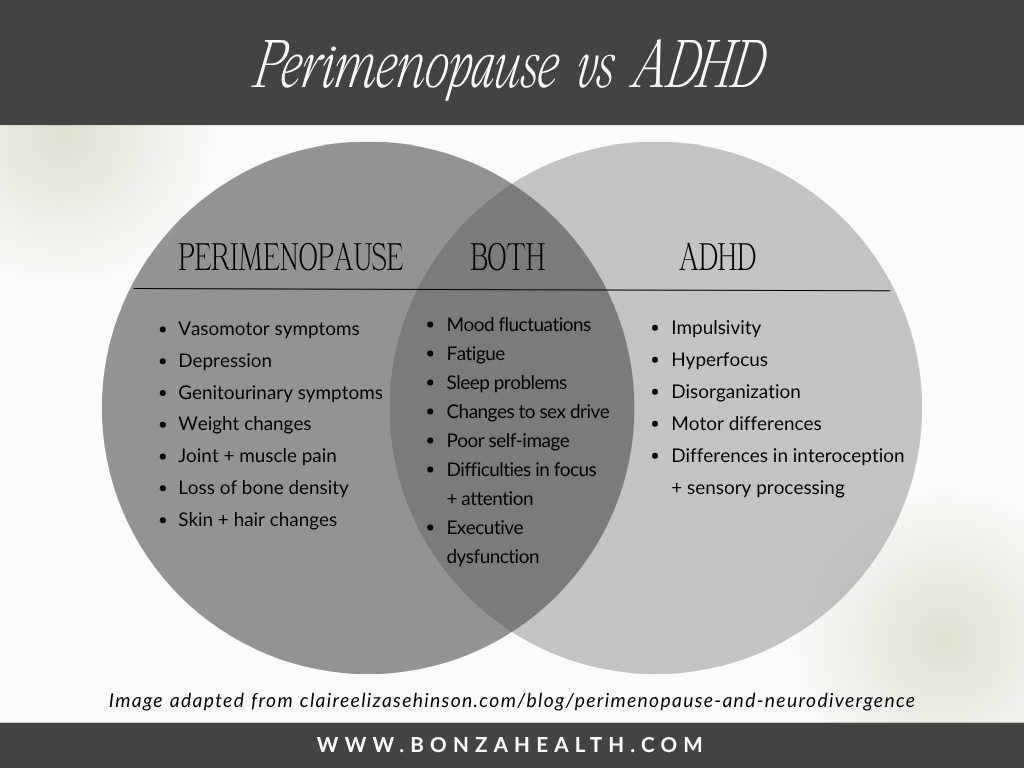
Perimenopause vs ADHD
The traditional medicine view: when stimulants are the answer
Conventional treatment for ADHD remains psychostimulant medication, and it works — including in midlife women. A small but illuminating study showed lisdexamfetamine improved executive function in perimenopausal and early postmenopausal women, even those without a formal ADHD diagnosis.⁴ There's also growing interest in coordinating ADHD treatment with hormone therapy: if estrogen modulates dopamine, then estrogen replacement may improve both menopausal cognition and ADHD medication response.
The takeaway: if symptoms are significantly impairing your work, relationships, or quality of life, a formal evaluation matters. Self-diagnosis from TikTok is a starting point, not an endpoint.

Conventional treatment for ADHD remains psychostimulant medication.
Lifestyle medicine: the daily inputs that move the needle
Before — or alongside — medication, the lifestyle inputs that affect dopaminergic function in midlife are not optional:
Caffeine, used strategically. Caffeine is a non-selective adenosine receptor antagonist, which increases dopamine signaling in the striatum and prefrontal cortex.⁵ For ADHD brains, modest, well-timed caffeine can support attention. The trap is using more of it to compensate for poor sleep, which fragments sleep further and worsens next-day cognition. A morning coffee: helpful. A 3 p.m. latte plus an afternoon energy drink: counterproductive.
The Mediterranean diet pattern. Multiple systematic reviews link Mediterranean-style eating — high in olive oil, fish, nuts, vegetables, and legumes — to slower cognitive decline and improved executive function.⁶ The mechanisms include omega-3 sufficiency, lower neuroinflammation, and steadier blood glucose, all of which support dopaminergic neurons.
Sleep, as treatment. Perimenopausal sleep is biologically harder. But deep sleep is when the brain consolidates memory and clears metabolic waste, and chronic deprivation worsens every ADHD and brain-fog symptom on the list. Protecting sleep is not a wellness platitude here — it's foundational.
Strength training.Resistance training raises BDNF (brain-derived neurotrophic factor) and supports dopaminergic tone. It also addresses bone loss, sarcopenia, and cognition simultaneously — uniquely valuable in midlife.

Multiple systematic reviews link Mediterranean-style eating to slower cognitive decline and improved executive function.
Functional medicine: methylation, MTHFR, and the folate story
Here, the conversation gets more nuanced. The MTHFR gene encodes an enzyme that converts folate into its active form, which is then required for methylation — a chemical process essential for synthesizing dopamine, serotonin, and norepinephrine.⁷
Two common MTHFR polymorphisms — C677T and A1298C — reduce enzyme activity. A 2022 meta-analysis of 66 studies concluded that the A1298C variant is associated with ADHD, and other variants in the folate-homocysteine pathway may contribute to ADHD risk.⁸ Reduced MTHFR activity can also disrupt synthesis of tetrahydrobiopterin (BH4), a cofactor required to produce dopamine, norepinephrine, and serotonin.
Where does that leave us clinically? A few honest caveats:
Routine MTHFR testing is not standard of care, and mainstream medicine and functional medicine disagree about whether genetic testing changes outcomes for most patients. That said, eating folate-rich foods (leafy greens, legumes, asparagus, avocado) and ensuring adequate B12, B6, and choline supports methylation regardless of genotype. For women with a known MTHFR polymorphism, persistent symptoms, or a history of depression that has not responded well to standard SSRIs, methylated B-vitamin support (methylfolate, methylcobalamin) is worth a conversation with a knowledgeable provider — not a self-directed experiment.

Eating folate-rich foods and ensuring adequate B12, B6, and choline supports methylation.
What about L-tyrosine?
L-tyrosine has become popular in the ADHD and perimenopause space because it's the amino acid precursor to dopamine and norepinephrine. The reasoning is intuitive: more substrate, more neurotransmitter.
The actual evidence is more modest than the marketing. Systematic reviews of L-tyrosine in healthy adults show acute, short-term cognitive benefits — but specifically under conditions of stress, sleep deprivation, or unusually high cognitive demand.⁹ There is no strong evidence that chronic L-tyrosine supplementation treats ADHD the way stimulant medication does, and individual response varies based on dopamine-receptor genetics (DRD2 variants).
Practical translation: L-tyrosine is generally safe at food-equivalent doses, and some women find it useful for demanding cognitive days. It is not a substitute for a thorough workup, hormone evaluation, or — when indicated — proper ADHD treatment. If you want to try it, work with a clinician who can monitor and contextualize.

L-tyrosine has become popular in the ADHD and perimenopause space because it's the amino acid precursor to dopamine and norepinephrine.
When to seek professional help
If you're nodding along to most of this, here is the threshold I use in practice. Any of these warrants a real conversation:
Symptoms are interfering with work performance, parenting, finances, or relationships.
You're leaning on compensatory strategies (extra caffeine, alcohol to wind down, sacrificing sleep) that are creating new problems.
A close family member has ADHD.
You suspect you've been masking your whole life and can no longer keep up.
Mood, anxiety, or sleep have shifted alongside the cognitive changes.
Look for a clinician who understands both midlife hormonal transitions and adult ADHD. That combined lens is still rare, but increasingly available.
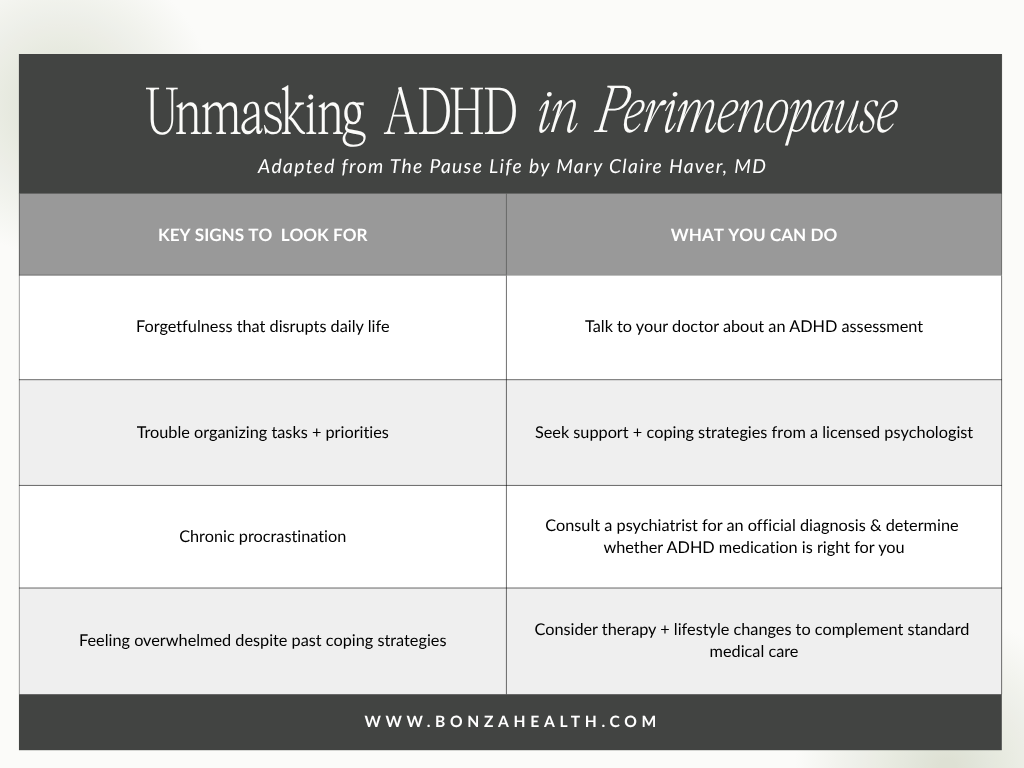
Unmasking ADHD in perimenopause
The bottom line
The "is it ADHD or perimenopause?" wave isn't a fad. It reflects a generation of women who were missed as children, now navigating a hormonal transition that pulls back the curtain on what was always there. The right answer is rarely one thing. It's a careful combination — sometimes hormone therapy, sometimes stimulants, always sleep and nutrition and movement, occasionally targeted nutrients — built around the specific woman in front of you.
You are not broken. You are not late. Your brain has changed, and it's asking for a different set of inputs than it used to need. That is worth listening to.

A traditional, lifestyle, and functional medicine approach to ADHD and perimenopause
References (PubMed)
Integrative literature review – the impact of ADHD across women's lifespan. PMC12683802. https://doi.org/10.1186/s12905-025-04123-1
Hidalgo-Lopez E, et al. ADHD and Sex Hormones in Females: A Systematic Review. PMC12145478. https://doi.org/10.1177/10870547251332319
Research advances and future directions in female ADHD: the lifelong interplay of hormonal fluctuations with mood, cognition, and disease. PMC12277363. https://doi.org/10.3389/fgwh.2025.1613628
Antoniou E, et al. Midlife ADHD in women: any relevance to menopause? PubMed 26914101. https://doi.org/10.3109/13697137.2016.1152536
Kahathuduwa CN, et al. The Cognitive-Enhancing Outcomes of Caffeine and L-theanine: A Systematic Review. PMC8794723. https://doi.org/10.7759/cureus.20828
Fu J, et al. Association between the Mediterranean diet and cognitive health among healthy adults: A systematic review and meta-analysis. PMC9372716. https://doi.org/10.3389/fnut.2022.946361
Wan L, et al. Methylenetetrahydrofolate reductase and psychiatric diseases. PMC6218441. https://doi.org/10.1038/s41398-018-0276-6
MTHFR Gene Polymorphisms: A Single Gene with Wide-Ranging Clinical Implications—A Review. PMC12027316. https://doi.org/10.3390/genes16040441
Bryant J, et al. Behavioral and cognitive effects of tyrosine intake in healthy human adults. PubMed 25797188. https://doi.org/10.1016/j.pbb.2015.03.008