
Why FSH Is Not a Reliable Indicator of Perimenopause—And What Is
Written and edited by Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

In the context of established postmenopause, an elevated FSH is a reliable biomarker. In perimenopause, it is not.
Many women entering perimenopause are told by their clinicians that a single follicle-stimulating hormone (FSH) blood test will determine whether they are in the menopausal transition and whether they are candidates for menopause hormone therapy (MHT). This practice is widespread, but it is not supported by current evidence or by leading menopause guidelines. Understanding why requires a clear look at what FSH is, how it behaves during perimenopause, and what measures actually correlate with both menopausal status and the likelihood of benefit from treatment.
Why a Single FSH Measurement Cannot Diagnose Perimenopause
The defining feature of perimenopause is hormonal variability, not steady decline. Ovarian function during the transition oscillates rather than tapers. Some cycles are ovulatory and others are anovulatory, follicular recruitment becomes irregular, and inhibin B and estradiol fluctuate substantially — sometimes within a single cycle. FSH tracks this variability in real time.
Burger's foundational analysis of FSH, estradiol, and inhibin across the menopausal transition demonstrated that FSH can rise abruptly into the postmenopausal range and then fall back to values typical of young fertile women, often while ovulatory cycles continue to occur [1]. Santoro and colleagues similarly documented that perimenopausal women show wide within-subject variation in FSH, luteinizing hormone, and estradiol, including episodes of both hyperestrogenism and hypergonadotropism that a single lab draw would not predict [2].
The statistical consequence of this variability has been quantified. In a reliability study of repeated FSH measurements, the intraclass correlation coefficient (a measure of how well repeated measurements on the same person agree) was 0.70 in postmenopausal women but only 0.09 in premenopausal women [3]. An ICC of 0.09 means a single FSH value in a premenopausal or early-perimenopausal woman provides essentially no reliable information about her true average FSH — repeat measurements are required for any meaningful interpretation.
For these reasons, the Stages of Reproductive Aging Workshop +10 (STRAW+10) — the international consensus framework for staging reproductive aging — specifies menstrual bleeding patterns as the primary criterion for staging the menopausal transition, with hormonal measurements (including FSH, anti-Müllerian hormone, inhibin B, and antral follicle count) serving only as supportive criteria [4]. No single FSH value places a woman in a STRAW+10 stage.
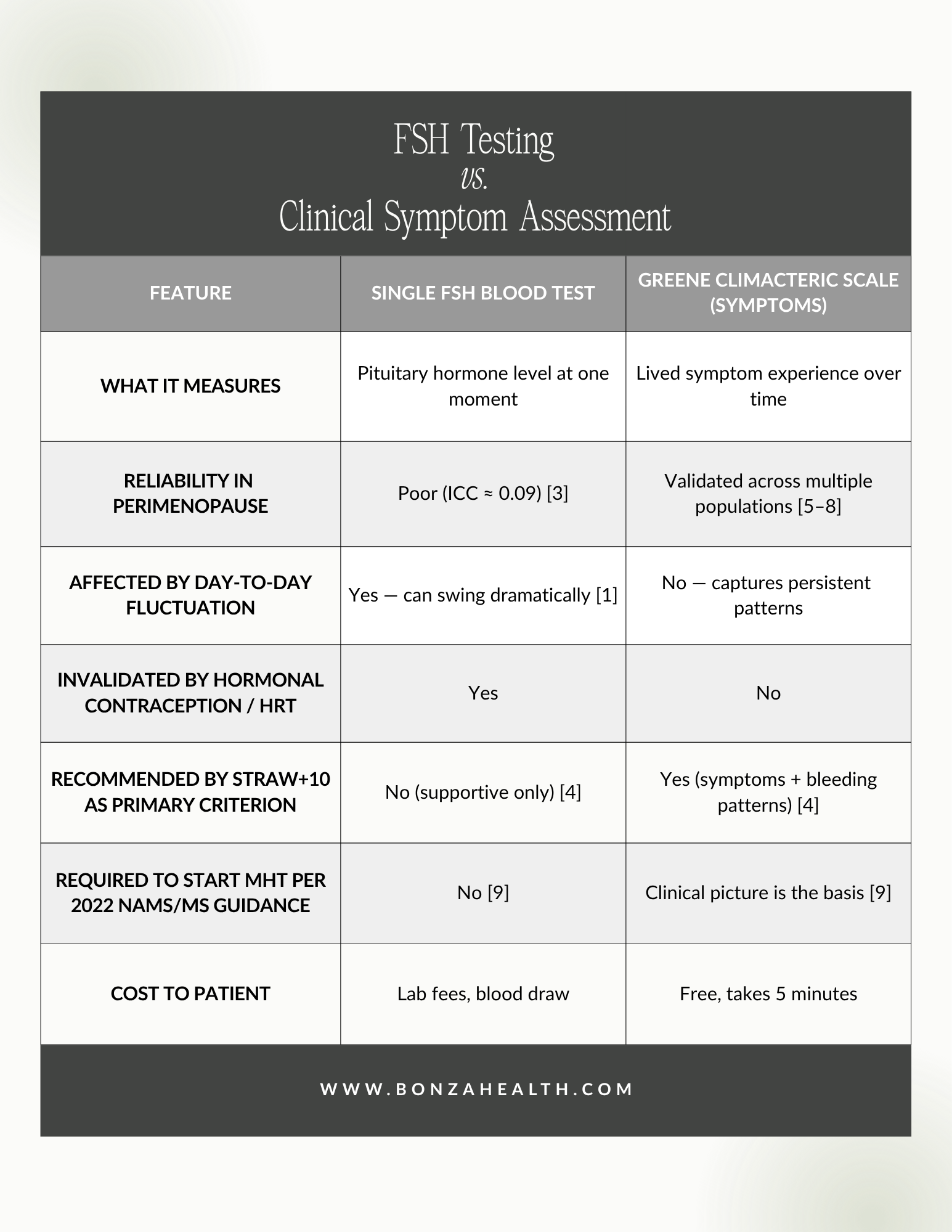
FSH Testing vs. Clinical Symptom Assessment
Why Clinical Symptoms Are a More Reliable Indicator
The hormonal variability of perimenopause produces a consistent and recognizable constellation of symptoms — vasomotor, psychological, somatic, and urogenital. Because these symptoms reflect the cumulative physiologic effects of fluctuating hormones over weeks and months, they are considerably more stable and clinically meaningful than any single hormone value.
The Greene Climacteric Scale (GCS) is a 21-item self-report instrument developed by J.G. Greene in 1998 from a consensus of seven prior factor-analytic studies of menopausal symptoms [5]. It measures four validated domains:
Psychological: Anxiety, irritability, depressive symptoms, difficulty concentrating, feeling unhappy, crying spells.
Somatic: Headaches, muscle and joint pain, paresthesias (numbness or tingling), dizziness, fatigue, and breathing difficulties.
Vasomotor: Hot flashes and night sweats.
Sexual: Loss of libido.
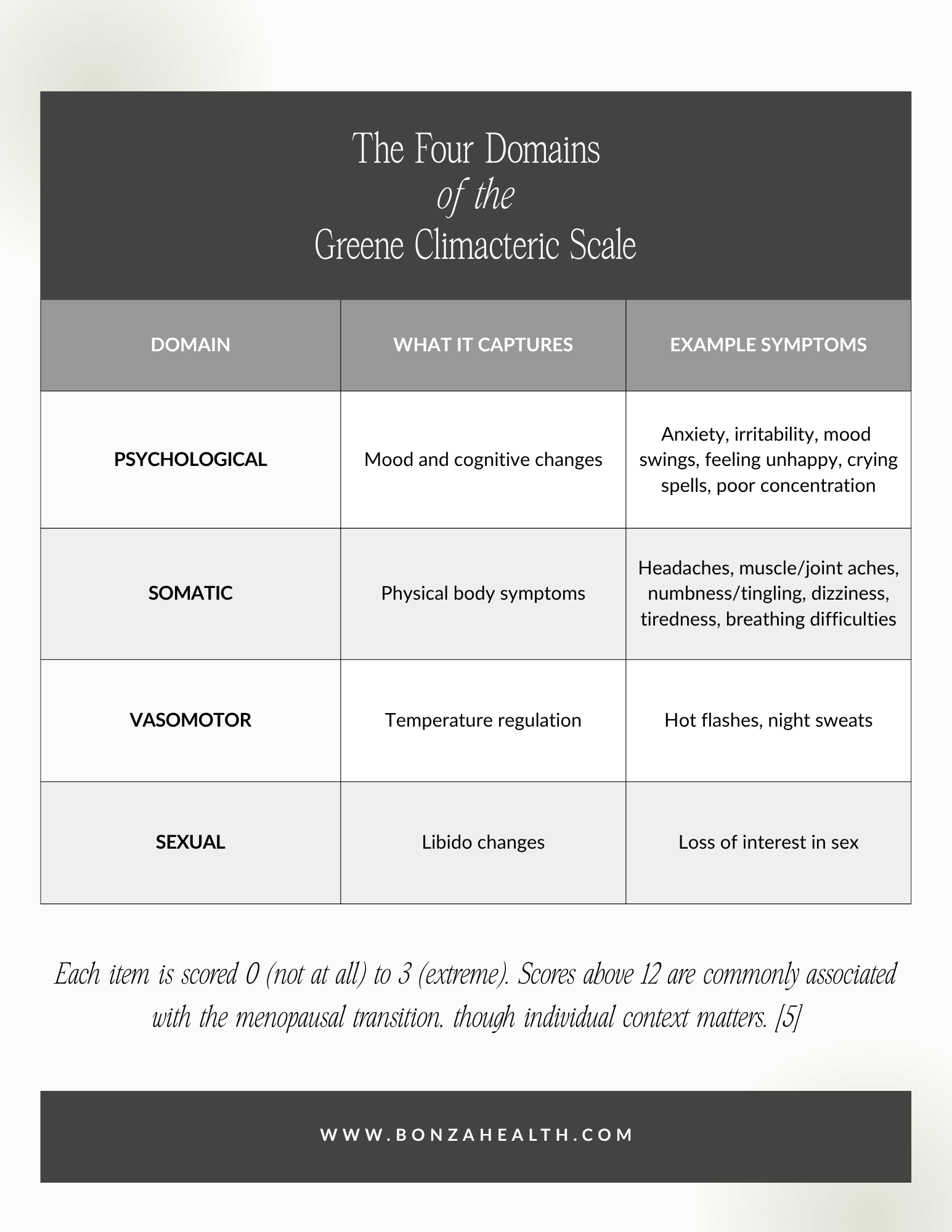
The Four Domains of the Greene Climacteric Scale [5]
Each item is rated from 0 (not at all) to 3 (extreme), producing a total score and four subscale scores. Population-based studies consistently demonstrate that GCS total scores rise significantly from premenopause (mean ~10) to perimenopause (mean ~15–16) and remain elevated in postmenopause [6,7]. A 2022 comparative analysis of four major menopausal symptom instruments — the GCS, Menopause Rating Scale, Kupperman Index, and Women's Health Questionnaire — found correlations exceeding 0.90 across instruments, confirming that the GCS reliably captures the same clinical construct measured by other validated tools [8].
Clinically, the GCS does something FSH cannot: it reflects the cumulative, lived experience of hormonal change rather than a snapshot of one moment — and it is the lived experience that is treated.
![Expected GCS Total Scores by Menopausal Stage [6]](https://images.squarespace-cdn.com/content/v1/63e20422289a555372cd45e4/50fa4543-bda1-4045-9043-207442c12e96/3.png)
Expected GCS Total Scores by Menopausal Stage [6]
What the Evidence Says About Initiating MHT
Current guidelines align treatment decisions with symptoms, not with a single laboratory threshold. The 2022 Menopause Society (formerly NAMS) Hormone Therapy Position Statement states that hormone therapy remains the most effective treatment for vasomotor symptoms and genitourinary syndrome of menopause, and that the benefit-risk profile is favorable for most healthy symptomatic women under age 60 or within 10 years of menopause onset. The same statement explicitly notes that routine serum hormone testing is rarely needed to guide MHT decisions [9].
In clinical terms: MHT candidacy is determined by symptom burden, age, time since final menstrual period, and individual risk factors — not by whether FSH has crossed a particular threshold on a particular day.

Current guidelines align treatment decisions with symptoms, not with a single laboratory threshold.
How to Advocate for Yourself in a Clinical Setting
If you have been told that your FSH is "normal" and therefore you are not a candidate for evaluation or treatment, the following steps are reasonable and evidence-aligned:
1. Bring documented symptom data. Complete a Greene Climacteric Scale (freely available online) and track your symptoms over 2–4 weeks. Bring the scored result to your appointment. A documented symptom score is more clinically actionable than a verbal description.
2. Use precise clinical terminology. Phrasing such as "I am experiencing vasomotor, psychological, and somatic symptoms consistent with the menopausal transition per STRAW+10 criteria" locates your experience within an accepted clinical framework.
3. Reference current guidelines. You can ask directly: "Per the 2022 Menopause Society Hormone Therapy Position Statement, hormone therapy is symptom-driven and routine hormone testing is not required. Can we discuss treatment based on my symptom profile?"
4. Request clinical rationale in writing. If MHT is declined, it is reasonable to request that the clinical reasoning be documented in your chart. This is a standard patient request and often prompts a more thorough evaluation.
5. Consider a menopause-certified clinician. The Menopause Society maintains a directory of practitioners credentialed in menopausal medicine (MSCP credential). These clinicians are specifically trained in symptom-based assessment and evidence-based MHT.
6. Seek a second opinion when appropriate. Dismissal of perimenopausal symptoms is well documented in the clinical literature and is not a standard of care that patients are obligated to accept.

Dismissal of perimenopausal symptoms is well documented in the clinical literature and is not a standard of care that patients are obligated to accept.
What This Means for You
FSH is a useful biomarker in specific clinical contexts, but a single FSH measurement cannot reliably diagnose perimenopause or determine candidacy for hormone therapy. The hormonal variability that defines the menopausal transition makes any single lab draw statistically unreliable [1,3]. International staging criteria (STRAW+10) and current hormone therapy guidelines (2022 Menopause Society Position Statement) both emphasize clinical symptoms and history as primary, with hormonal testing as supportive at most [4,9]. Validated symptom instruments such as the Greene Climacteric Scale provide a more accurate, reproducible, and clinically meaningful characterization of the menopausal transition [5,8] — and a stronger foundation for individualized, shared decision-making about treatment.
If your symptoms are consistent with perimenopause and a "normal" FSH has been used to deny you further evaluation, the current evidence supports advocating for a symptom-based clinical assessment.

Dr. Sarah Bonza, MD, is the founder of Bonza Health, where she partners with women navigating perimenopause and menopause using evidence-based, individualized care. Schedule a consultation at www.bonzahealth.com.
References
[1] H. G. Burger, "Diagnostic role of follicle-stimulating hormone (FSH) measurements during the menopausal transition—an analysis of FSH, oestradiol and inhibin," Hum. Reprod., vol. 9, Suppl. 2, pp. 9–16, 1994. PMID: 8124478.
[2] N. Santoro, J. R. Brown, T. Adel, and J. H. Skurnick, "Characterization of reproductive hormonal dynamics in the perimenopause," J. Clin. Endocrinol. Metab., vol. 81, no. 4, pp. 1495–1501, Apr. 1996. PMID: 8636357.
[3] A. Zeleniuch-Jacquotte, R. E. Shore, Y. Afanasyeva, et al., "Reliability of follicle-stimulating hormone measurements in serum," Reprod. Biol. Endocrinol., vol. 1, art. 49, 2003. PMCID: PMC165593.
[4] S. D. Harlow, M. Gass, J. E. Hall, et al., "Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging," J. Clin. Endocrinol. Metab., vol. 97, no. 4, pp. 1159–1168, Apr. 2012. PMID: 22344196.
[5] J. G. Greene, "Constructing a standard climacteric scale," Maturitas, vol. 29, no. 1, pp. 25–31, May 1998. PMID: 9643514.
[6] R. Barentsen, P. H. van de Weijer, S. J. van Gend, and H. Foekema, "Climacteric symptoms in a representative Dutch population sample as measured with the Greene Climacteric Scale," Maturitas, vol. 38, no. 2, pp. 123–128, Apr. 2001. PMID: 11306200.
[7] C. Travers, S. M. O'Neill, R. King, D. Battistutta, and S. K. Khoo, "Greene Climacteric Scale: norms in an Australian population in relation to age and menopausal status," Climacteric, vol. 8, no. 1, pp. 56–62, Mar. 2005. PMID: 15804732.
[8] A. Monterrosa-Castro, V. Paternina-Caicedo, and P. Chedraui, "Correlation among four questionnaires that evaluate menopausal symptoms," Menopause, vol. 29, no. 9, pp. 1076–1082, Sep. 2022. PMID: 35674650.
[9] The NAMS 2022 Hormone Therapy Position Statement Advisory Panel, "The 2022 hormone therapy position statement of The North American Menopause Society," Menopause, vol. 29, no. 7, pp. 767–794, Jul. 2022. PMID: 35797481.