
Oxytocin for Perimenopause: The "Love Hormone" That May Help Libido, Mood, and Vaginal Atrophy
Written and edited by Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Oxytocin is not just about emotional bonding. It is a wide-acting neuropeptide whose role in midlife women is still being mapped.
A patient came into my office recently. Forty-seven, two children, married twenty years. She had read an article that suggested oxytocin nasal spray could "save her marriage." She wasn't sleeping well. Sex had become uncomfortable, then infrequent, then a source of quiet grief between her and her husband. Her primary care doctor had told her she was "fine for her age." Her labs were unremarkable. She wanted to know if the article was right.
This is the conversation I'm having more and more often. Women in perimenopause are encountering oxytocin online — usually framed as the "love hormone" or the "cuddle hormone" — and they want to know whether it's something real, or just the next wellness trend with a clinical-sounding name.
The honest answer is: somewhere in between. There is a real, peer-reviewed evidence base for certain applications of oxytocin in midlife women. There is also a great deal of marketing that runs well ahead of the data. As a board-certified menopause-trained physician, my job is to help you tell the difference.
Here is what I actually think about oxytocin in perimenopause, where the evidence holds up, where it doesn't, and how I think about it in my own practice.
What oxytocin actually is (and what it isn't)
Oxytocin is a nine–amino-acid peptide hormone produced in the hypothalamus and released by the posterior pituitary gland. Most of us learned about it in two contexts: labor and breastfeeding. Synthetic oxytocin (Pitocin) has been used clinically for more than fifty years to induce contractions and support milk letdown.
What we didn't learn in medical school is that oxytocin receptors are found throughout the body — in the brain, the cardiovascular system, the gut, the bones, the skin, and the vaginal epithelium. This receptor distribution is the reason oxytocin has been investigated for an unusually wide range of conditions: chronic pain, social anxiety, postpartum depression, autism spectrum traits, gastroparesis, weight regulation, and — most relevant to us — sexual function and vaginal tissue health in women.
So when someone calls it the "love hormone," that name is accurate but incomplete. Oxytocin is not just about emotional bonding. It is a wide-acting neuropeptide whose role in midlife women is still being mapped.

Oxytocin receptors are found throughout the body: in the brain, the cardiovascular system, the gut, the bones, the skin, and the vaginal epithelium.
Why oxytocin is suddenly relevant in perimenopause
Three things are happening at once.
First, estrogen decline during perimenopause changes the vaginal epithelium, the autonomic nervous system, and the brain regions involved in mood and sexual response. The symptoms that result — vaginal dryness, painful intercourse, low libido, anxiety, sleep disruption, difficulty with emotional regulation — are real and undertreated.
Second, many women cannot or will not use traditional hormone therapy. Some have contraindications. Some are uncertain about the data. Some have tried it and want adjunctive options.
Third, the compounding pharmacy industry has made oxytocin available in formulations that didn't exist a generation ago: intranasal sprays, sublingual troches, and vaginal creams. This availability has created both real clinical opportunity and a marketplace that is, frankly, ahead of the evidence in places.
The question is not whether oxytocin "works." The question is: for what, in whom, and how strong is the evidence.

Estrogen decline during perimenopause changes the vaginal epithelium, the autonomic nervous system, and the brain regions involved in mood and sexual response.
The evidence: where it's strongest, where it's weaker
Let me walk through the three areas most relevant to perimenopausal women, in order of how confident I am in the data.
1. Vaginal atrophy: the strongest evidence
This is, in my reading, where the data on oxytocin is most compelling.
The genitourinary syndrome of menopause (GSM) — what we used to call vaginal atrophy — affects an estimated 50–90% of postmenopausal women. The vaginal epithelium thins, pH rises, lubrication decreases, and intercourse can become painful. Standard treatment is local vaginal estrogen, which is safe and effective for the vast majority of women. But not every patient can or wants to use it, and for those women, the evidence on oxytocin gel has grown surprisingly robust over the past decade.
The story begins with a research group in Sweden led by Shahla Al-Saqi and Kerstin Uvnäs-Moberg. In their 2015 randomized, double-blind, placebo-controlled trial, they compared 400 IU and 100 IU vaginal oxytocin gel against placebo in postmenopausal women over seven weeks [1]. The 400 IU dose produced statistically significant improvements in vaginal cell maturation and patient-reported symptoms, prompting the authors to suggest that intravaginal oxytocin "could be an alternative to local estrogen treatment." The same group followed up the next year with a larger 68-woman multicenter trial, which confirmed those findings on both cytological and histological examination — meaning oxytocin appeared to improve the vaginal mucosa not just by surface measures but at the tissue level [2].
An independent Iranian trial in 2020 tested 400 IU oxytocin vaginal gel nightly in 96 postmenopausal women and again demonstrated significant improvement in subjective symptoms, vaginal pH, and the maturation index after 30 days of treatment [3]. A 2023 systematic review and meta-analysis pooled the available randomized trials and concluded that oxytocin gel showed measurable benefit over placebo for the symptoms of GSM [4].
Keep in mind, oxytocin is not clearly as effective as estrogen — local vaginal estrogen remains the most studied and most effective therapy for GSM — but for women who cannot or prefer not to use estrogen, vaginal oxytocin is one of the more evidence-supported non-hormonal options available through compounding pharmacies today.

The genitourinary syndrome of menopause (GSM) — what we used to call vaginal atrophy — affects an estimated 50–90% of postmenopausal women.
2. Sexual function and libido: more complicated than the marketing suggests
This is where I want to slow down, because this is also where oxytocin is most aggressively marketed online.
The most often-cited investigation of intranasal oxytocin for female sexual dysfunction is Dana Muin and colleagues' 2015 randomized, double-blind, placebo-controlled crossover trial in Fertility and Sterility [5]. Thirty pre- and postmenopausal women with sexual dysfunction self-administered 32 IU of intranasal oxytocin or placebo within 50 minutes before intercourse, over a 22-week period, with crossover between the two arms midway through.
The findings deserve to be quoted carefully. After oxytocin, Female Sexual Function Index (FSFI) scores increased by 26%; after placebo, they increased by 31%. Sexual Quality of Life scores rose 144% with oxytocin and 125% with placebo. Sexual Interest and Desire Inventory scores climbed 29% with oxytocin and 23% with placebo. Both groups improved meaningfully — but the placebo group improved at least as much as the oxytocin group, and the authors concluded that long-term intranasal oxytocin offered no significant treatment effect over placebo.
This does not mean oxytocin is useless for libido. It means the controlled evidence to date does not show it outperforms placebo in this setting. It also means the act of being in a study, paying focused attention to one's sexual life, and using any pre-intercourse ritual may be doing some of the therapeutic work that gets attributed to the medication itself.
Oxytocin should be prescribed as a potentially helpful adjunct within a thoughtful overall plan — one that may also include hormone therapy, attention to vaginal tissue health, relationship and mental health context, and rest. I do not promise it will work like a switch. The data simply does not support that promise.

It’s unclear whether oxytocin can support common mood-related symptoms of perimenopause.
3. Mood, anxiety, and emotional regulation: interesting signals, limited direct evidence in perimenopause
There is a substantial body of research on oxytocin in social cognition and mood, though almost none of it is conducted specifically in perimenopausal women. The clearest direct evidence comes from Guastella and colleagues' 2009 randomized controlled trial, which showed that intranasal oxytocin enhanced the effects of exposure therapy for social anxiety disorder [6]. A 2023 systematic review by Zhu, Jin, and Tang synthesized the randomized trial evidence for oxytocin in postpartum depression [7]. There is also exploratory research on oxytocin's role in stress regulation and emotional connection, and a small pilot study on oxytocin nasal spray in fibromyalgia — a condition that overlaps with perimenopausal pain syndromes in my practice more than the literature reflects [8].
What we don't have is a body of high-quality, perimenopause-specific randomized trials showing that intranasal oxytocin treats the mood symptoms of perimenopause. The mechanism is plausible — perimenopausal mood disturbance involves the same neurochemical systems on which oxytocin acts — but plausibility is not evidence.
In my practice, I treat perimenopausal mood symptoms first with the tools that do have strong evidence: appropriate hormone therapy when indicated, lifestyle medicine fundamentals, treatment of underlying anxiety or depression, and a careful look at sleep, alcohol use, and nutritional status. Oxytocin is a secondary consideration in this domain, not a first-line answer.
How oxytocin is supplied
Compounding pharmacies offer oxytocin in several formulations. The route matters because oxytocin is destroyed by digestive enzymes when taken orally, which is why effective administration is intranasal, sublingual/buccal, or intravaginal.

Oxytocin can be taken intranasally, sublingually/buccally, or intravaginally.
Suggested dosing ranges that have appeared in the published literature and clinical references include (these are reference points only, not prescriptions — actual dosing must be individualized):
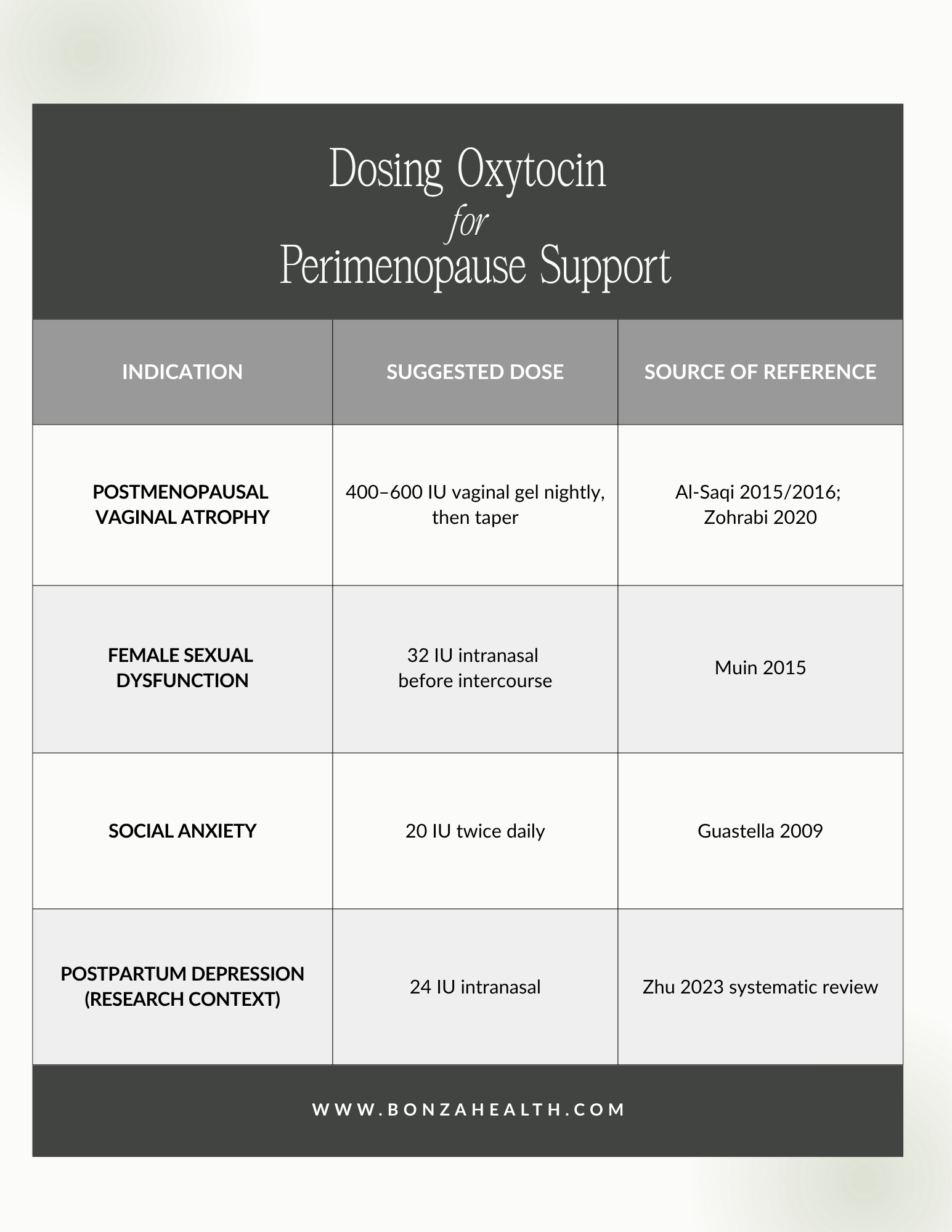
Note: These are reference points only, not a prescription. Actual dosing must be individualized.
Please keep in mind: oxytocin used in these compounded formulations is not FDA-approved for any of these indications. Compounded medications are prepared based on individual prescriptions and are not reviewed by the FDA for safety or efficacy in the way that brand-name medications are. That does not mean they cannot be appropriate — they often are — but it does mean the prescribing physician's judgment, monitoring, and informed consent process matters more, not less.
Who should not use compounded oxytocin
Even peptides that look gentle deserve a careful candidate screen.

Compounded oxytocin is not appropriate for every woman. Even peptides that appear gentle deserve a careful candidate screen.
Side effects most commonly reported include nausea, headache, dizziness, and nasal irritation with the spray formulation. Rarely, more significant effects can occur, which is why this is a prescription medication and not a supplement.
How oxytocin fits with hormone therapy
This is the question I get asked most often. Should I use oxytocin instead of hormone therapy?
For most women experiencing perimenopausal symptoms, that framing is the wrong question. Menopause hormone therapy (MHT), when appropriate, addresses the underlying hormonal shift that is driving the constellation of perimenopausal symptoms. Oxytocin is a peptide acting on specific receptor systems — it is a tool with specific applications, not a replacement for systemic hormonal support when that is indicated.
The way I think about it clinically:
Vaginal estrogen is the gold standard for GSM. Vaginal oxytocin is a reasonable consideration for women who cannot or prefer not to use vaginal estrogen, or as a complement in selected cases.
Systemic MHT addresses the foundational hormonal shifts of perimenopause. Intranasal oxytocin may have a place as an adjunct for specific symptoms (mood, libido) in carefully selected patients, with the understanding that the evidence base for these uses is weaker than for vaginal atrophy.
Lifestyle medicine fundamentals — sleep, strength training, protein intake, alcohol moderation, stress regulation — remain the foundation regardless of which medications are layered on top. I write about this often because it matters.

Menopause hormone therapy (MHT), when appropriate, addresses the underlying hormonal shift that is driving the constellation of perimenopausal symptoms.
My honest take
Oxytocin is one of the more interesting peptides in midlife women's health, and the vaginal atrophy data, in particular, is worth taking seriously. It is also one of the most over-promised compounds in the wellness-medical marketplace, and patients deserve a clinician who is willing to tell them where the evidence ends.
If you are a perimenopausal woman struggling with vaginal dryness, painful intercourse, or low libido, the right next step is not to order something online. It is to sit down with a physician who can take a full history, look at your hormonal picture, talk through your goals and constraints, and decide together whether something like oxytocin — alone or in combination with hormone therapy — actually fits your situation.
That is the conversation I am here to have.
Ready to talk through what's actually happening — and what might help?
If this article describes you, I'd love to help you sort through your options.
→ Take the Bonza Health hormone quiz to see if a consultation is a good fit.
→ Book a 50-minute consultation with Dr. Bonza — we'll look at your full picture, discuss whether peptides, hormone therapy, or both make sense, and build a plan that's actually personalized to you.
Related reading on Bonza Health:

Dr. Sarah Bonza, MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC is a board-certified Family Physician and Certified Menopause Practitioner serving women in Ohio and beyond. Bonza Health is licensed to practice in Ohio. Compounded peptide medications, including oxytocin formulations, are prescribed only after thorough clinical evaluation and informed consent.
This article is for educational purposes and does not constitute medical advice. Compounded medications, including those discussed here, are not FDA-approved for the indications described and should be used only under the direction of a qualified, licensed healthcare provider.
References
The studies cited below are available through PubMed and the publishers' websites. I encourage curious readers to look at the abstracts themselves — bringing questions to your appointment is something I genuinely welcome.
[1] S. H. Al-Saqi, K. Uvnäs-Moberg, and A. F. Jonasson, "Intravaginally applied oxytocin improves post-menopausal vaginal atrophy," Post Reprod. Health, vol. 21, no. 3, pp. 88–97, Sep. 2015, https://doi.org/10.1177/2053369115577328
[2] S. H. Al-Saqi, A. F. Jonasson, T. Naessen, and K. Uvnäs-Moberg, "Oxytocin improves cytological and histological profiles of vaginal atrophy in postmenopausal women," Post Reprod. Health, vol. 22, no. 1, pp. 25–33, 2016, https://doi.org/10.1177/2053369116629042
[3] I. Zohrabi, P. Abedi, S. Ansari, E. Maraghi, N. Shakiba Maram, and G. Houshmand, "The effect of oxytocin vaginal gel on vaginal atrophy in postmenopausal women: A randomized controlled trial," BMC Women's Health, vol. 20, no. 1, art. 108, May 2020, https://doi.org/10.1186/s12905-020-00935-5
[4] R. A. Farahat, H. M. Salamah, A. Mahmoud, et al., "The efficacy of oxytocin gel in postmenopausal women with vaginal atrophy: An updated systematic review and meta-analysis," BMC Women's Health, vol. 23, no. 1, art. 494, Sep. 2023, https://doi.org/10.1186/s12905-023-02645-0
[5] D. A. Muin, M. Wolzt, R. Marculescu, et al., "Effect of long-term intranasal oxytocin on sexual dysfunction in premenopausal and postmenopausal women: A randomized trial," Fertil. Steril., vol. 104, no. 3, pp. 715–723.e4, Sep. 2015, https://doi.org/10.1016/j.fertnstert.2015.06.010
[6] A. J. Guastella, A. L. Howard, M. R. Dadds, P. Mitchell, and D. S. Carson, "A randomized controlled trial of intranasal oxytocin as an adjunct to exposure therapy for social anxiety disorder," Psychoneuroendocrinology, vol. 34, no. 6, pp. 917–923, Jul. 2009, https://doi.org/10.1016/j.psyneuen.2009.01.005
[7] J. Zhu, J. Jin, and J. Tang, "Oxytocin and women postpartum depression: A systematic review of randomized controlled trials," Neuropsychiatr. Dis. Treat., vol. 19, pp. 939–947, Apr. 2023, https://doi.org/10.2147/NDT.S393499
[8] S. Mameli, G. M. Pisanu, S. Sardo, et al., "Oxytocin nasal spray in fibromyalgic patients," Rheumatol. Int., vol. 34, no. 8, pp. 1047–1052, Aug. 2014, https://doi.org/10.1007/s00296-014-2953-y