
Navigating the Intersection of PCOS & Perimenopause
Written and edited by Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

Understanding the Compounded Metabolic Crisis and Why Early Action Matters
Polycystic ovary syndrome (PCOS) is one of the most prevalent endocrine disorders affecting women of reproductive age, impacting an estimated 8-13% of women worldwide [1]. For decades, it has been framed primarily as a fertility issue. But PCOS is, at its core, a lifelong metabolic condition, and nowhere does that become more apparent than when it collides with perimenopause.
Perimenopause, the transitional phase preceding menopause, typically spanning 4 to 10 years, brings its own cascade of hormonal disruption. When these two conditions converge, the metabolic consequences can be profound and, if unrecognized, dangerous. As a physician, I see this intersection far too often go unaddressed until it evolves into frank metabolic syndrome, type 2 diabetes, or cardiovascular disease.
This blog is for the woman who has been told she 'may outgrow her PCOS': you haven't. It is for the woman entering her 40s, noticing new weight gain, worsening insulin resistance, and irregular cycles being dismissed as 'just perimenopause.' Your body is telling you something. Let's listen.
What Is PCOS? A Metabolic Disorder in Disguise
PCOS is defined by a combination of hyperandrogenism (excess male-type hormones), ovulatory dysfunction, and polycystic ovarian morphology on ultrasound. However, its diagnosis is nuanced, with different consensus criteria varying in emphasis:
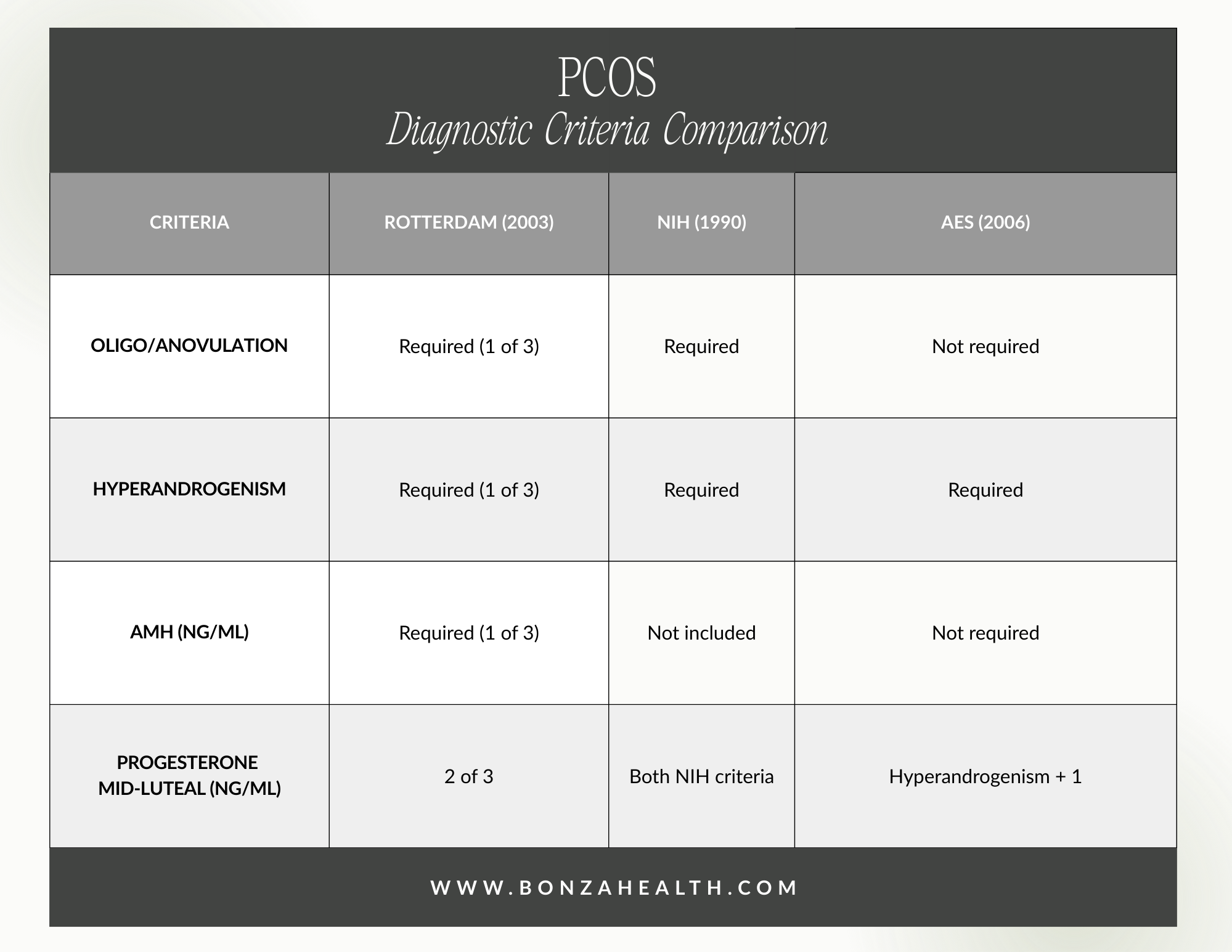
PCOS Diagnostic Criteria Comparison
Beyond reproductive manifestations, PCOS is strongly associated with insulin resistance (IR)—present in 50-70% of affected women—regardless of body weight [2]. This hyperinsulinemic state directly stimulates ovarian androgen production, worsening the hormonal milieu and contributing to anovulation, acne, hirsutism, and weight gain. The physiological dysfunction is circular and self-reinforcing.
Perimenopause: A Hormonal Tipping Point
During perimenopause, estrogen levels fluctuate erratically before declining, progesterone production falls, and the hypothalamic-pituitary-ovarian axis becomes increasingly dysregulated. These changes have significant metabolic consequences of their own:
Fat Redistribution: Increased visceral adiposity as estrogen-protective effects on fat distribution wane
Impaired Insulin Sensitivity: declining estrogen worsens pancreatic beta-cell function and peripheral glucose uptake
Adverse Lipid Changes: LDL rises, HDL falls, and triglycerides increase, elevating cardiovascular risk
Blood Pressure Dysregulation: Disrupted estrogen affects cortisol regulation and sympathetic tone, raising blood pressure
Reduced Lean Muscle Mass: falling estrogen and androgen shifts impair muscle protein synthesis
In women without PCOS, these changes are challenging enough. In women with PCOS, who already carry an elevated metabolic burden, perimenopause acts as an accelerant—pushing a smoldering metabolic fire into a full blaze.

PCOS is one of the most prevalent endocrine disorders affecting women of reproductive age, impacting an estimated 8-13% of women worldwide [1].
The Compounded Risk: When PCOS Meets Perimenopause
The hormonal overlap between these two conditions is complex. Women with PCOS have characteristically elevated luteinizing hormone (LH) and testosterone, and relatively low progesterone. As perimenopause begins, FSH rises erratically, estradiol fluctuates, and the ovaries—already dysfunctional in PCOS—struggle to respond. The result is a worsening of all pre-existing metabolic vulnerabilities [3].
A particularly important consideration is that the relative hyperandrogenism of PCOS may persist longer into perimenopause than in healthy women. While testosterone naturally declines with age in all women, the disproportionately elevated baseline in PCOS means women may continue to experience clinical hyperandrogenism—including hirsutism, acne, and androgenic alopecia—well into their 40s and 50s [4].
Clinically, this means a perimenopausal woman with PCOS may present with hot flashes, irregular periods, AND ongoing acne and hair thinning. This combination can be confusing to both patient and provider, but it is entirely consistent with the pathophysiology of PCOS in the menopausal transition.
Metabolic Syndrome: The Danger Downstream
Metabolic syndrome—defined by the presence of at least three of five criteria (central obesity, elevated fasting glucose, elevated triglycerides, reduced HDL, and hypertension)—is the key downstream risk. Women with PCOS already have a 2-3x higher risk of metabolic syndrome compared to age-matched controls [5]. Perimenopause adds additional risk, creating a compounded burden that demands early, proactive clinical attention.
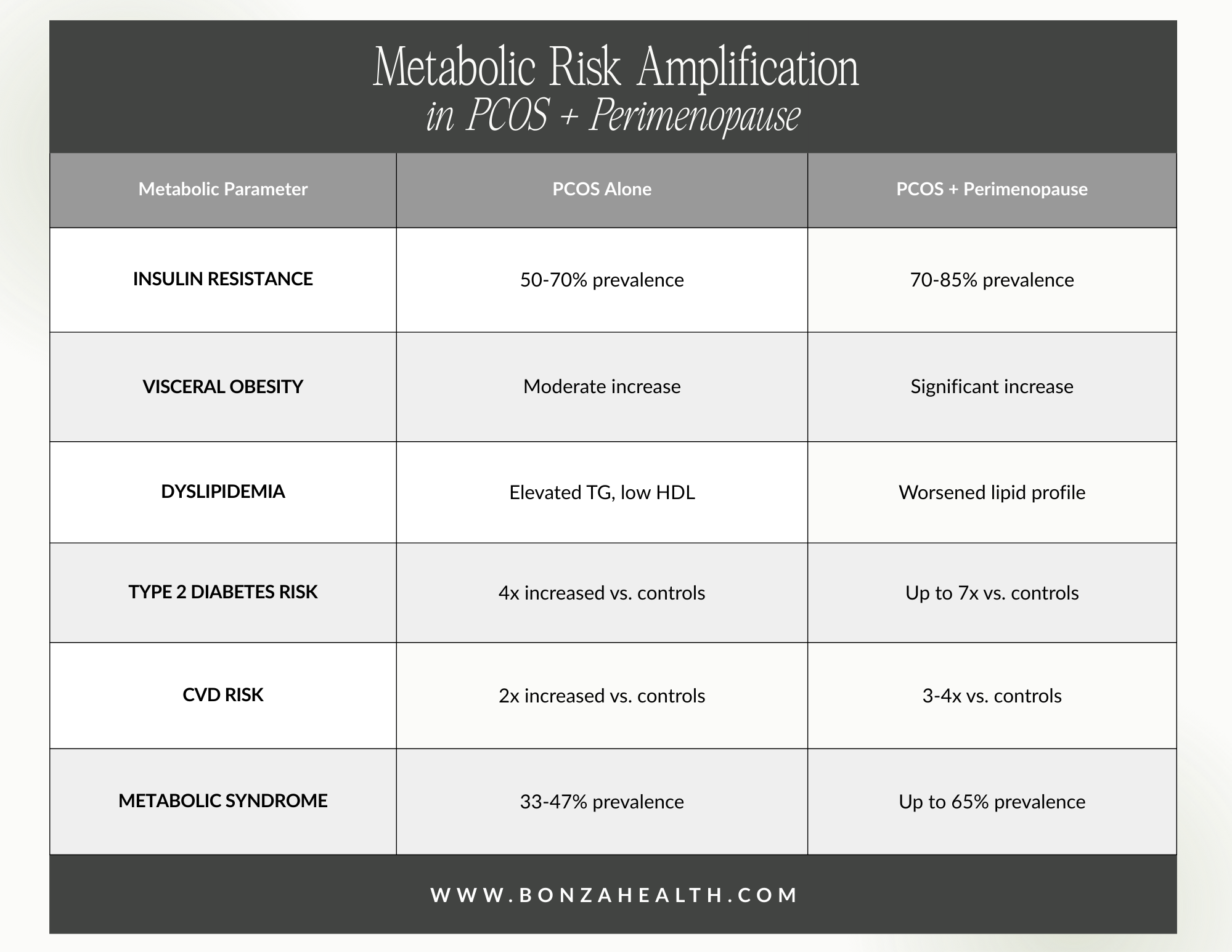
Metabolic Risk Amplification in PCOS + Perimenopause
The cardiovascular implications are serious. Studies demonstrate that women with PCOS have a 2-fold increased risk of cardiovascular events compared to controls, and perimenopause amplifies this further through adverse lipid changes, endothelial dysfunction, and systemic inflammation [6]. Alarmingly, many of these women are never formally screened for metabolic syndrome during routine gynecological or primary care visits.
Anovulation, Infertility, and the Hormonal Rollercoaster
Anovulation—the failure to release an egg—is a hallmark of PCOS due to LH/FSH ratio dysregulation and elevated androgens, which impair follicular maturation. In perimenopause, anovulatory cycles become the norm as ovarian follicular reserve depletes. For women with PCOS, this creates a paradoxical clinical challenge: they may experience prolonged irregular or absent periods that mirror both their existing PCOS pattern and typical perimenopausal cycling changes [7].
For women in their late 30s to mid-40s who still wish to conceive, this convergence is critical. PCOS already reduces fecundity through anovulation and endometrial dysfunction; perimenopause further reduces ovarian reserve and egg quality. Women with PCOS who delay pregnancy should be counseled about ovarian reserve testing (AMH, antral follicle count) starting in their early 30s and about reproductive options proactively.
Additionally, women with PCOS on oral contraceptives—a common management strategy—may have menopausal symptoms masked by exogenous hormones. Clinicians must consider transitioning these patients off OCPs temporarily to assess hormonal status, particularly in the late 40s, and pivot toward menopause hormone therapy (MHT) as appropriate.
A Framework for Early Intervention
The guiding principle in managing PCOS through perimenopause is this: do not wait for disease to declare itself. Treat the terrain. The goal is to aggressively address insulin resistance, maintain healthy body composition, protect cardiovascular health, and manage symptoms of both PCOS and the menopausal transition simultaneously.
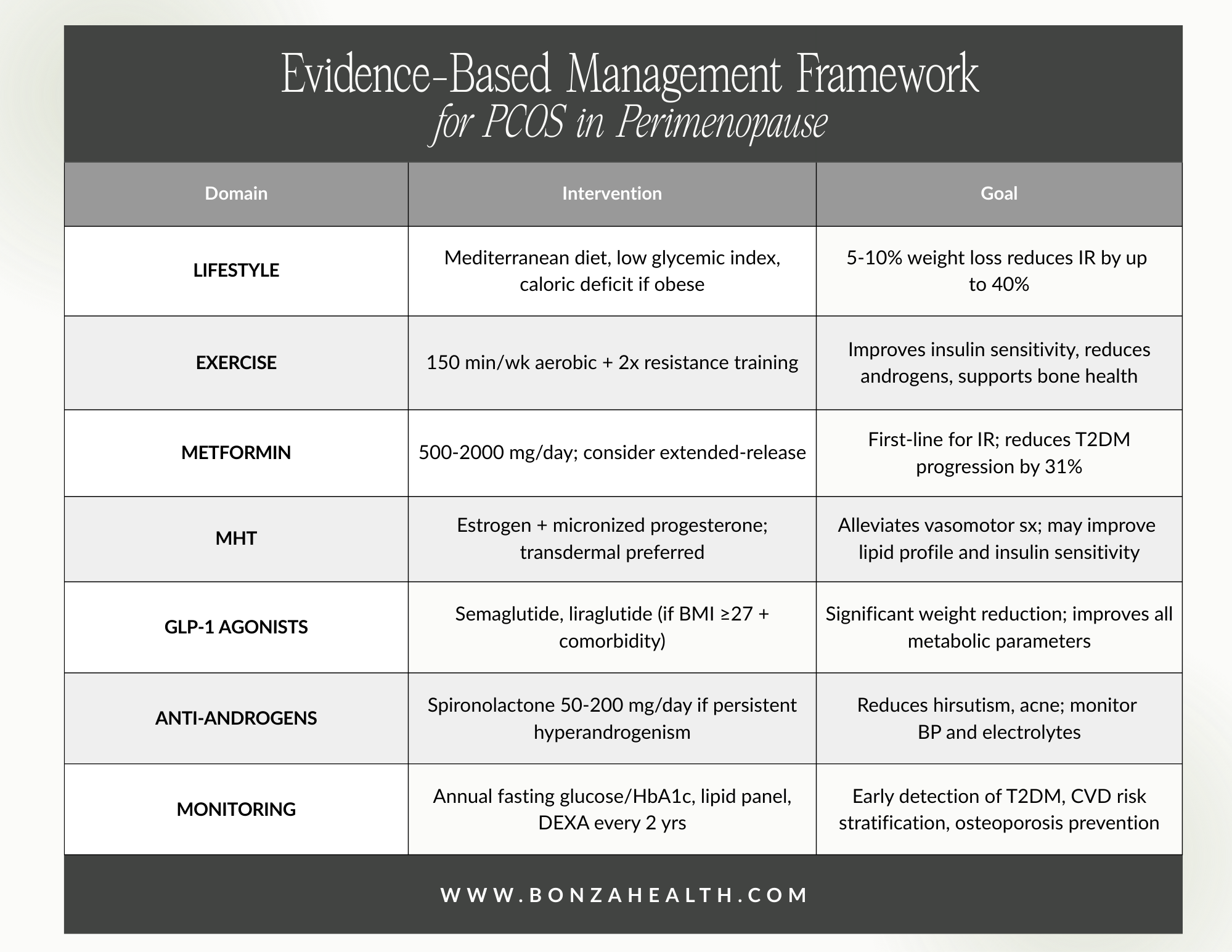
Evidence-Based Management Framework for PCOS in Perimenopause
A special note on Menopause Hormone Therapy (MHT): women with PCOS are often estrogen-dominant earlier in life due to anovulatory cycles and relative progesterone deficiency. As perimenopause progresses, however, estrogen falls and the calculus shifts. Transdermal estradiol with micronized progesterone (rather than synthetic progestins) is the preferred formulation, offering favorable metabolic and cardiovascular profiles. MHT in appropriate candidates can improve insulin sensitivity, lipid profiles, sleep, and quality of life, and should not be reflexively withheld from PCOS patients [8].
Lifestyle Medicine: The Non-Negotiable Foundation
No pharmacological strategy substitutes for lifestyle intervention. In both PCOS and menopause research, lifestyle medicine consistently demonstrates the most durable metabolic benefit:
Nutrition: A Mediterranean-style, low-glycemic diet reduces fasting insulin, lowers testosterone levels, and supports weight loss. Avoid ultra-processed foods, refined carbohydrates, and added sugars: the key drivers of hyperinsulinemia.
Exercise: A combination of aerobic activity and resistance training is superior to either alone. Resistance training is especially important in perimenopause for preserving lean muscle mass and improving glucose disposal. Aim for 150 minutes of moderate aerobic activity plus 2 strength sessions weekly.
Sleep Optimization: Chronic sleep deprivation worsens insulin resistance, elevates cortisol, and increases appetite-stimulating hormones. Women with PCOS and perimenopause are at high risk for sleep-disordered breathing and insomnia; screen and treat aggressively.
Stress Reduction: Chronic psychological stress perpetuates HPA axis dysregulation, elevates cortisol and androgens, and worsens insulin resistance. Mindfulness-based stress reduction (MBSR), yoga, and cognitive behavioral therapy (CBT) have evidence in both populations.
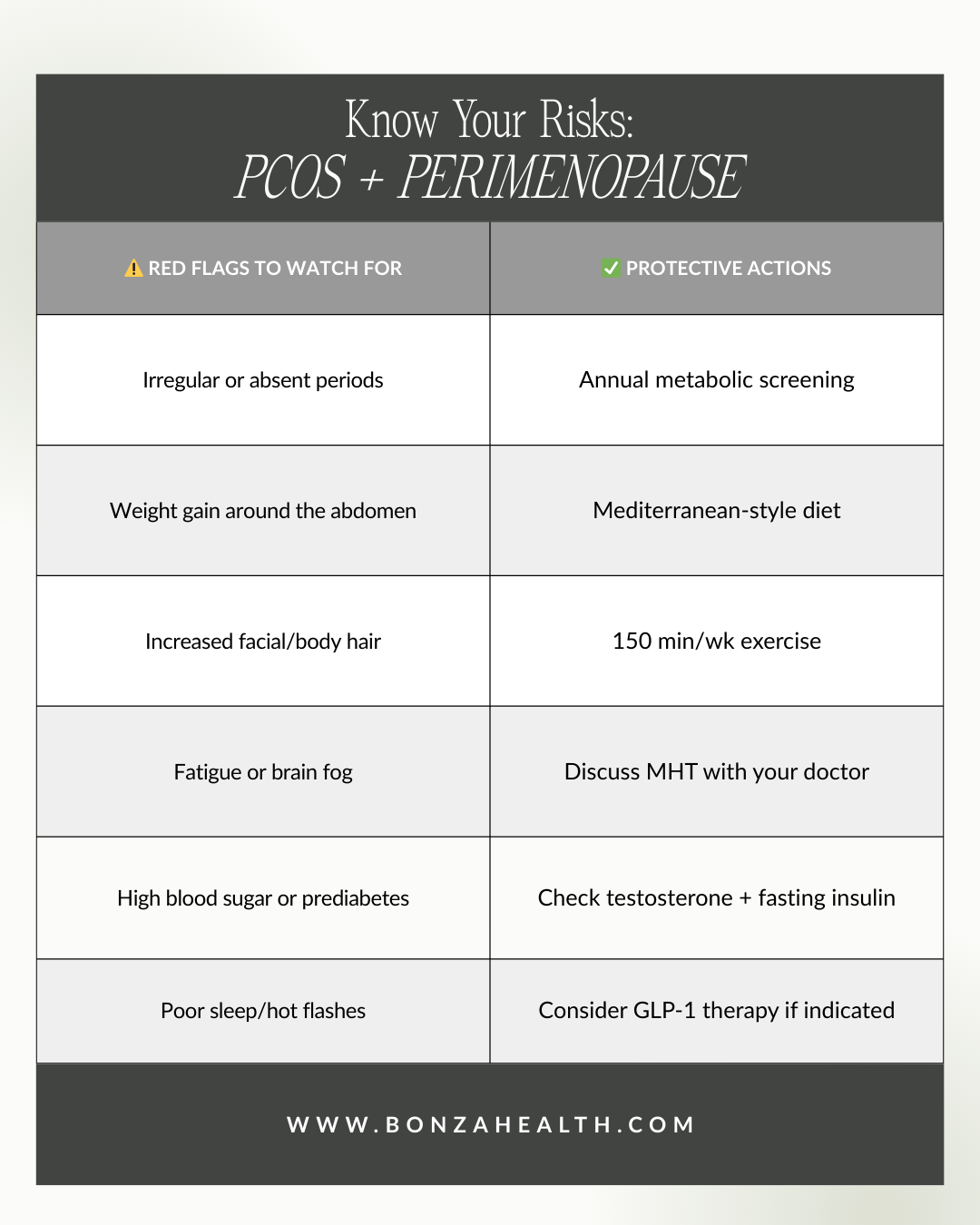
Know your risks: PCOS and perimenopause
Conclusion: Advocate for Your Metabolic Health
PCOS does not simply 'go away' with age. The reproductive chapter may close, but the metabolic story continues—and perimenopause writes some of its most consequential pages. Women navigating this intersection deserve providers who understand the compounded risks, who screen proactively, and who offer evidence-based, individualized interventions that address the whole person.
If you have PCOS and are approaching or in perimenopause, advocate for:
Annual fasting glucose, HbA1c, fasting insulin, and lipid panel
Testosterone (total and free), SHBG assessment
Blood pressure monitoring at every visit
Discussion of MHT candidacy with a menopause-trained provider
Referral to a dietitian and certified exercise specialist with metabolic expertise
The window for prevention is open. Let us not wait until metabolic syndrome, type 2 diabetes, or cardiovascular disease forces our hand. Intervene early. Treat the terrain. And empower women to understand their bodies at every stage.

Book your consult with Dr. Bonza to start reclaiming your health in perimenopause
References
S. Bozdag, S. Mumusoglu, D. Zengin, E. Karabulut, and B. O. Yildiz, "The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis," Hum. Reprod., vol. 31, no. 12, pp. 2841-2855, 2016.
R. S. Legro, A. R. Kunselman, W. C. Dodson, and A. Dunaif, "Prevalence and predictors of risk for type 2 diabetes mellitus and impaired glucose tolerance in polycystic ovary syndrome: a prospective, controlled study in 254 affected women," J. Clin. Endocrinol. Metab., vol. 84, no. 1, pp. 165-169, 1999.
J. Lizneva, D. Gavrilova-Jordan, W. Walker, and R. Azziz, "Androgen excess: Investigations and management," Best Pract. Res. Clin. Obstet. Gynaecol., vol. 37, pp. 98-118, 2016.
E. C. Crespo, H. O. Villagomez, R. Azziz, and E. Carmina, "Evolution of clinical and hormonal features in women with polycystic ovary syndrome: a longitudinal study," Fertil. Steril., vol. 113, no. 6, pp. 1229-1237, 2020.
R. A. Wild, E. Carmina, E. Diamanti-Kandarakis, A. Dokras, H. F. Escobar-Morreale, W. Futterweit, R. Lobo, R. J. Norman, E. Talbott, and R. S. Legro, "Assessment of cardiovascular risk and prevention of cardiovascular disease in women with the polycystic ovary syndrome: a consensus statement by the Androgen Excess and Polycystic Ovary Syndrome (AE-PCOS) Society," J. Clin. Endocrinol. Metab., vol. 95, no. 5, pp. 2038-2049, 2010.
J. E. Shaw, R. A. Sicree, and P. Z. Zimmet, "Global estimates of the prevalence of diabetes for 2010 and 2030," Diabetes Res. Clin. Pract., vol. 87, no. 1, pp. 4-14, 2010.
H. Teede, M. Deeks, and L. Moran, "Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan," BMC Med., vol. 8, no. 41, 2010.
The Menopause Society, "The 2023 Menopause Society Position Statement on Hormone Therapy in Postmenopausal Women," Menopause, vol. 30, no. 6, pp. 573-590, 2023.
R. J. Norman, D. Dewailly, R. S. Legro, and T. E. Hickey, "Polycystic ovary syndrome," Lancet, vol. 370, no. 9588, pp. 685-697, 2007.
J. Rosenfield and D. Ehrmann, "The pathogenesis of polycystic ovary syndrome (PCOS): the hypothesis of PCOS as functional ovarian hyperandrogenism revisited," Endocr. Rev., vol. 37, no. 5, pp. 467-520, 2016.