
The Hidden Value of Lab Testing in Perimenopause: A Clinical Perspective on Prescribing Hormone Therapy
Written and edited by Sarah Bonza MD, MPH, FAAFP, MSCP, DipABLM, NBC-HWC

The hidden value of lab testing in perimenopause
If you've been told your labs are "normal" while experiencing brain fog, night sweats, crippling anxiety, or sleep disturbances, you're not imagining things. You are not crazy. And you're certainly not alone.
At Bonza Health, we hear this story constantly: women in their late 30s, 40s, and early 50s who know something has changed in their bodies seek help from their healthcare providers, only to be told that because their FSH isn't elevated or their estradiol looks "fine," they don't need hormone therapy. They're sent home with suggestions to reduce stress, exercise more, or consider an antidepressant.
Here's what traditional medical practice often gets wrong: lab values in perimenopause are inherently variable, and "normal" ranges were often established using populations that don't reflect your individual physiology.
In this article, I want to share a different perspective: one grounded in evidence but also in the clinical reality of treating hundreds of perimenopausal women. Lab testing can be valuable. And understanding how to interpret those labs, including often-overlooked markers like progesterone, testosterone, and SHBG, can make the difference between getting the help you need and being dismissed.
The Traditional View: "Labs Aren't Needed"
Let me be transparent about what the guidelines say. Organizations like NICE (National Institute for Health and Care Excellence), ACOG, and even The Menopause Society state that routine hormone testing is not required to diagnose perimenopause in women over 45 with typical symptoms [1]. The reasoning is sound in a population-health sense: FSH and estradiol fluctuate so dramatically during perimenopause that a single measurement may be misleading.
The STRAW+10 criteria, the gold standard staging system for reproductive aging, explicitly notes that "due to the significant variation in hormone levels, measurements of FSH and estradiol are not routinely indicated to diagnose menopause" [2]. This is technically correct.
But here's what this guidance misses: diagnosing perimenopause is not the same as treating perimenopause. And labs, when properly timed and interpreted, can provide crucial information for tailoring treatment to your specific hormonal picture.
Understanding the Key Hormone Markers
Let's examine each hormone marker and what it can, and cannot, tell us about where you are in the menopausal transition and what treatment might help.
Anti-Müllerian Hormone (AMH): Your Ovarian Reserve Clock
AMH is produced by the granulosa cells of developing ovarian follicles. Unlike FSH and estradiol, AMH remains relatively stable throughout the menstrual cycle, making it easier to interpret regardless of when it's drawn [3].
What AMH tells us: AMH reflects your remaining ovarian follicle pool: essentially, how many eggs you have left. Studies show that AMH is a stronger predictor of time to menopause than FSH, especially in women with values below 1 ng/mL [4]. The SWAN study demonstrated that low AMH (<10 pg/mL) predicts a 51-79% probability of reaching the final menstrual period within 12 months, depending on age [5].
Clinical utility: When AMH is very low or undetectable, it tells us you're likely in late perimenopause, even if your FSH hasn't skyrocketed yet. This information can guide treatment decisions; for example, continuous combined hormone therapy may be more appropriate than cyclic regimens.

Follicle-Stimulating Hormone (FSH): The Classic (But Complicated) Marker
FSH is produced by the pituitary gland and stimulates ovarian follicle development. As ovarian reserve declines, FSH rises: it's the brain's attempt to "turn up the volume" on quiet ovaries.
The timing trap: Here's where traditional practice often fails women. FSH should ideally be drawn on cycle days 2-5 (early follicular phase) for the most accurate reading [6]. An elevated FSH (>25 IU/L) suggests late menopausal transition per STRAW+10 criteria [2]. However, and this is critical, a normal FSH does NOT rule out perimenopause.
Why? Because in early perimenopause, estradiol can actually be elevated (more on this below), which suppresses FSH through negative feedback. Your FSH may look perfectly normal while your hormonal rollercoaster is in full swing.
Clinical pearl: A single normal FSH in a symptomatic 40-45 year old woman will be elevated in a preceding or subsequent cycle about 30% of the time [6]. If symptoms strongly suggest perimenopause, consider repeating the test.

Luteinizing Hormone (LH): The Supporting Player
LH is less useful as a standalone marker but changes later than FSH during the menopausal transition. The LH:FSH ratio inverts as menopause approaches, but this isn't routinely used in clinical practice. Its primary value is confirming patterns seen with other markers and understanding ovulation timing.

Estradiol (E2): The Paradox of Perimenopause
Here's the information that changes everything for many women: estradiol levels during perimenopause average 20-30% HIGHER than premenopausal levels [2,7]. Read that again.
The common misconception that perimenopause is simply a time of estrogen decline is only partly true. In early perimenopause, chaotic hypothalamic-pituitary-ovarian feedback leads to erratic estrogen spikes, not deficiency [8]. Some women describe feeling pregnant—breast tenderness, nausea, emotional volatility—because their estrogen is soaring unpredictably.
The estrogen drop comes later: Estradiol doesn't decline significantly until 1-2 years before the final menstrual period, and doesn't stabilize until about 2 years afterward [2].
Timing matters enormously: Estradiol varies dramatically across the menstrual cycle. Drawing it randomly can give wildly different results. For clinical decision-making, early follicular phase (days 2-5) provides the most useful baseline. Values >80 pg/mL in this window may suppress what would otherwise be an elevated FSH [6].

Progesterone: The Forgotten Hormone of Perimenopause
If there's one hormone that deserves more attention in perimenopause conversations, it's progesterone. While everyone focuses on estrogen, progesterone deficiency is often the first hormonal change in perimenopause, and it may be driving many of your symptoms [8].
Understanding progesterone production: Progesterone is produced by the corpus luteum, the temporary structure that forms after ovulation. No ovulation means no progesterone. As perimenopause begins, ovulation becomes inconsistent. You may have cycles where you ovulate and produce progesterone, and cycles where you don't (anovulatory cycles). This creates the hormonal chaos many women experience.
When and how to test progesterone: Unlike FSH and estradiol, progesterone must be tested during a specific window: the mid-luteal phase, approximately 7 days after ovulation (typically day 21 of a 28-day cycle, but adjusted for your actual cycle length) [9]. A progesterone level >3 ng/mL confirms ovulation occurred. Levels >10 ng/mL suggest adequate luteal function. Levels <3 ng/mL during this window indicates anovulation: you didn't release an egg that cycle.
The perimenopause progesterone pattern: In perimenopause, you may see:
Anovulatory cycles with very low progesterone (<1 ng/mL mid-luteal)
Short luteal phases (ovulation occurs, but progesterone drops too quickly)
Insufficient luteal phases (progesterone is produced but at inadequate levels, 3-7 ng/mL)
Symptoms of low progesterone: Anxiety, irritability, sleep disturbances (especially difficulty staying asleep), heavy or irregular periods, breast tenderness, water retention, mood swings, and decreased stress tolerance. Many women describe feeling "wired but tired."
Clinical importance: If your mid-luteal progesterone is consistently low (<3 ng/mL) or you're having anovulatory cycles, you have objective evidence of hormonal dysfunction, regardless of what your estradiol or FSH shows. This is precisely the situation where progesterone-only therapy may be beneficial.

Testosterone: The Overlooked Player in Women's Hormonal Health
Here's a fact that surprises most women: before menopause, your body produces approximately three times more testosterone than estrogen [10]. Yet testosterone is rarely discussed in perimenopause, and that's a significant oversight.
Testosterone production in women: Testosterone is produced by the ovaries, adrenal glands, and through peripheral conversion in tissues like fat and skin. Unlike the dramatic decline of estrogen at menopause, testosterone declines gradually starting in your late 20s. By midlife, levels may be 50% lower than at peak [11]. However, surgical menopause (removal of the ovaries) can cause an abrupt 50% drop.
Symptoms of low testosterone in women:
Low libido or decreased sexual desire
Persistent fatigue despite adequate sleep
Brain fog and difficulty concentrating
Loss of muscle mass and strength
Depression or flat mood
Decreased motivation and drive
Testing testosterone: Both total testosterone and free testosterone (the biologically active fraction) can be measured. Testing should ideally occur in the morning when levels peak. Normal premenopausal total testosterone ranges from approximately 15-70 ng/dL, though this varies by lab. Free testosterone is often more clinically relevant, with normal ranges typically 0.3-1.9 ng/dL [12].
Testosterone therapy for women: Current guidelines (including NICE 2024) support considering testosterone supplementation for menopausal women with low sexual desire when estrogen replacement alone hasn't been effective [1]. A 2024 pilot study of 510 women found that transdermal testosterone therapy improved not only libido but also mood, anxiety, and cognitive symptoms [13]. Therapy is typically administered as a transdermal gel or cream at approximately 1/10th the male dose, aiming to restore levels to the normal premenopausal range.
Important caveat: Testosterone therapy for women is considered "off-label" in the US, as there are no FDA-approved testosterone products specifically for women. However, it is supported by international guidelines and growing evidence when used appropriately under medical supervision [14].

Sex Hormone-Binding Globulin (SHBG): The Hidden Regulator
SHBG may be the most underappreciated lab marker in hormone testing. This protein, produced primarily by the liver, acts as a transport vehicle for sex hormones but does much more than simply carry them around.
Why SHBG matters: SHBG binds to testosterone and estradiol, making them inactive while bound. Only "free" or unbound hormones are biologically active and can affect your tissues [15]. This means two women with identical total testosterone levels can have very different symptoms depending on their SHBG levels.
High SHBG scenario: If your SHBG is high, more of your testosterone (and estrogen) is bound and inactive. Even with "normal" total hormone levels, you may experience symptoms of deficiency—low libido, fatigue, brain fog—because your free hormone levels are actually low.
Low SHBG scenario: If your SHBG is low, more hormone is free and active. This can lead to symptoms of androgen excess—acne, oily skin, unwanted hair growth—even with "normal" total testosterone.
What affects SHBG:
Estrogen increases SHBG (oral estrogen more than transdermal)
Insulin resistance and obesity decrease SHBG
Thyroid function affects SHBG (hyperthyroidism increases it)
Body weight strongly correlates with SHBG (higher BMI = lower SHBG) [16]
SHBG and metabolic health: The SWAN study found that increasing SHBG levels during the menopausal transition were associated with a 10% reduced risk of developing diabetes [17]. Low SHBG is independently associated with metabolic syndrome, cardiovascular risk, and insulin resistance, making it a valuable marker beyond reproductive health.
Clinical utility: When symptoms don't match hormone levels, SHBG often provides the missing piece. A woman with normal total testosterone but high SHBG and low libido may benefit from testosterone supplementation. SHBG testing is also valuable when monitoring oral versus transdermal hormone therapy, as oral estrogens significantly raise SHBG (which can bind up testosterone, worsening libido despite treating other symptoms).
Normal range: SHBG typically ranges from 18-144 nmol/L in women, though this varies by age and lab. Context matters more than the absolute number.
Why "Normal" Labs Don't Mean Normal Symptoms
Here's the clinical picture that labs often miss: you can have high estrogen AND be severely symptomatic because you're not ovulating and producing progesterone.
Dr. Jerilynn Prior, a leading researcher in perimenopause physiology, has emphasized this critical point: "The most symptomatic women have higher E2 and lower progesterone levels" [8]. The issue isn't just hormones being too high or too low: it's the relationship between hormones becoming uncoupled.
During normal cycles, ovulation produces progesterone for roughly 14 days, balancing estrogen's effects. But perimenopause brings:
Anovulatory cycles (no ovulation, no progesterone)
Short luteal phases (ovulation occurs, but progesterone is produced for fewer days)
Insufficient luteal phases (progesterone is produced for the right duration but in inadequate amounts)
Variable SHBG binding that affects how much free hormone reaches your tissues
This creates a state of "unopposed estrogen" and explains symptoms like heavy bleeding, breast tenderness, irritability, anxiety, and insomnia that can occur even when your estradiol looks normal or elevated. Add in declining testosterone, and the picture becomes even more complex.

Treatment Approaches: Matching Therapy to Your Hormonal Picture
Understanding your lab picture, along with your symptoms and cycle patterns, allows us to tailor treatment more precisely.
Progesterone-Only Therapy: When Estrogen Isn't the Problem
For women in early perimenopause with evidence of estrogen dominance (high or normal estradiol, anovulatory cycles, symptoms of progesterone deficiency), oral micronized progesterone (OMP) alone may be the most appropriate treatment [8,18].
Evidence supports progesterone-only therapy for:
Night sweats and hot flashes (300mg at bedtime showed 56% reduction in one RCT [19])
Sleep disturbances (progesterone enhances GABA receptor activity [8])
Heavy menstrual bleeding (regulates endometrial shedding)
Anxiety and mood instability
Breast tenderness
How it's prescribed: Cyclic progesterone (300mg at bedtime for the last 14 days of the menstrual cycle) or continuous low-dose progesterone (100-200mg nightly) depending on cycle regularity [20].

Cyclic/Sequential Estradiol Therapy: For Women Still Menstruating
When labs and symptoms suggest late perimenopause with declining estrogen (low-normal estradiol, elevated FSH, vasomotor symptoms), sequential hormone therapy may be appropriate [21,22].
How it works: Estradiol is taken continuously (patch, gel, or oral), with progesterone added for 12-14 days each month. This mimics the natural cycle and typically results in a predictable withdrawal bleed [22].
Important considerations: The 2024 International Menopause Society White Paper notes that "prescribing MHT in the perimenopause can be difficult because the fluctuations in hormone levels can result in episodes of estrogen deficiency rapidly followed by episodes of estrogen excess" [21]. This is why sequential regimens are preferred: they allow flexibility.

Adding Testosterone: When Standard HRT Isn't Enough
If you're on optimized estrogen/progesterone therapy but still experiencing persistent low libido, fatigue, brain fog, or low motivation, testosterone may be the missing piece.
Who might benefit:
Women with Hypoactive Sexual Desire Disorder (HSDD) not responsive to estrogen therapy
Women with surgical menopause (loss of ovarian testosterone production)
Women with persistent fatigue and cognitive symptoms despite adequate estrogen
Women with low total/free testosterone and high SHBG on labs
Approach: Transdermal testosterone (gel or cream) is preferred over oral forms. The goal is to restore levels to normal premenopausal ranges, not to exceed them. Monitoring every 6 months for clinical response and to screen for excess is recommended [14].
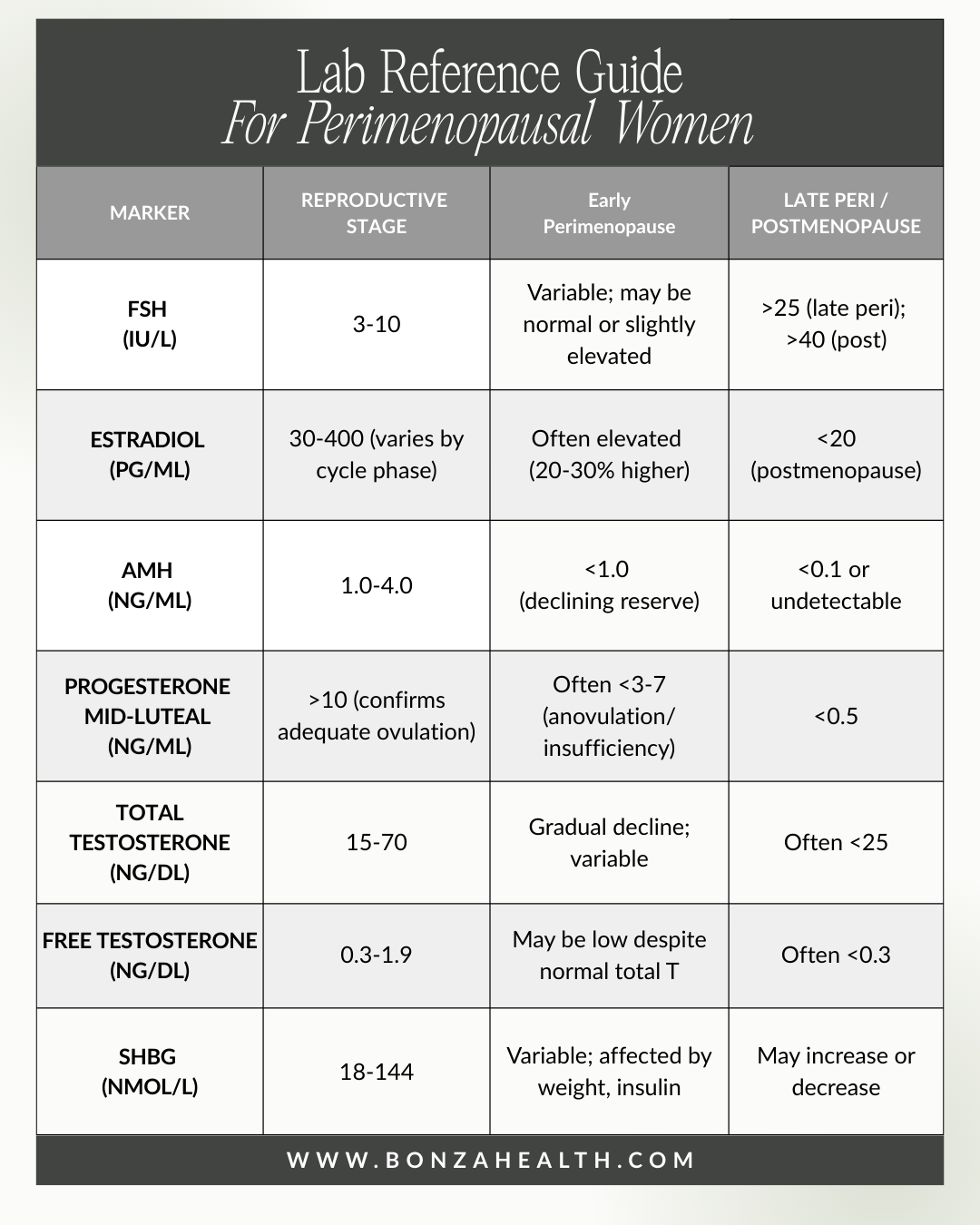
Note: These values are guidelines and must be interpreted in clinical context. Always draw FSH, estradiol, and SHBG on cycle days 2-5; progesterone on day 21 (or 7 days post-ovulation) for most accurate interpretation.
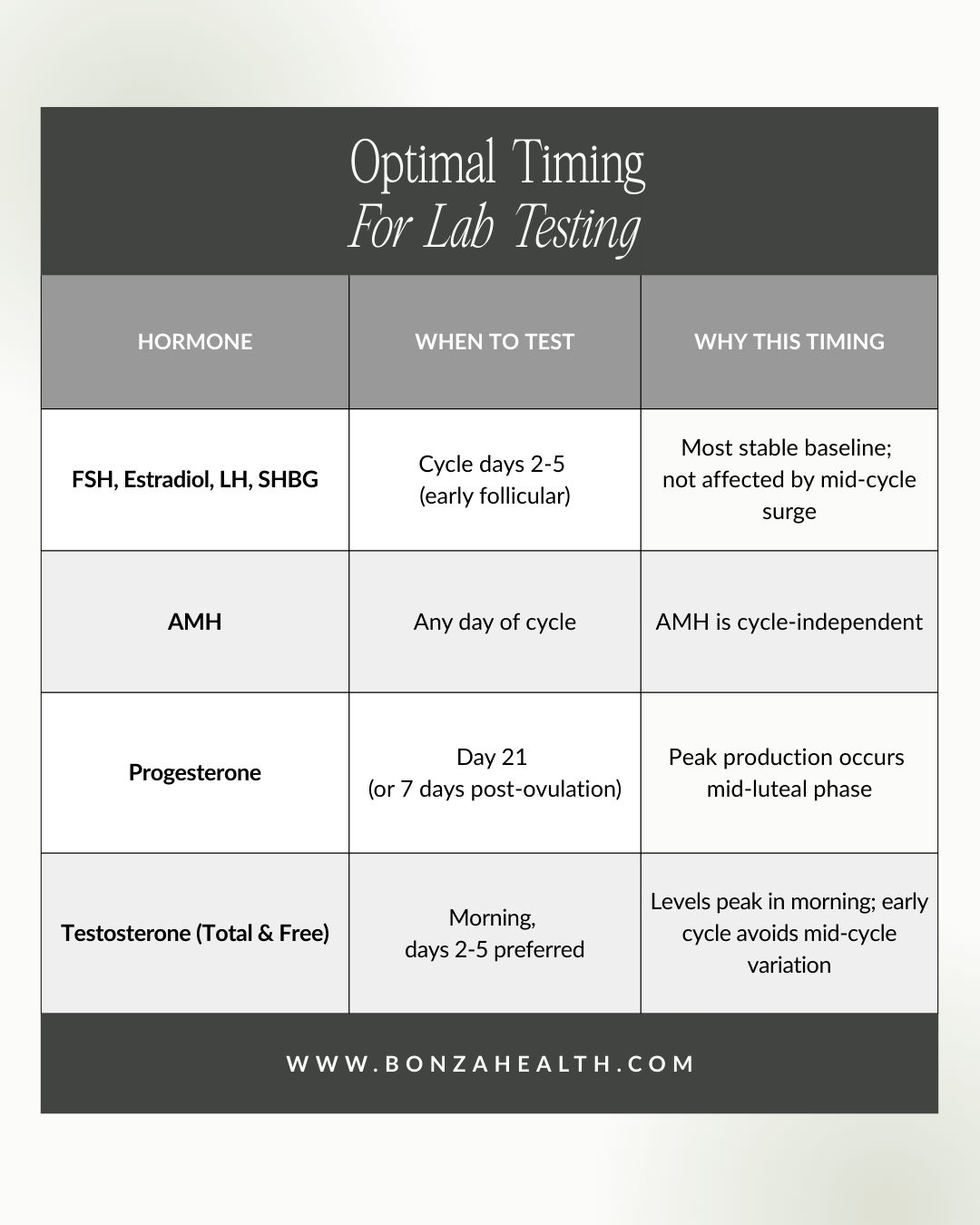
Optimal timing for lab testing
Practical Takeaways: Advocating for Yourself
What to ask your provider:
"Can we check a comprehensive hormone panel including FSH, estradiol, AMH, progesterone (mid-luteal), testosterone, and SHBG?"
"If my labs are normal but I'm symptomatic, can we discuss treatment options anyway?"
"Would progesterone-only therapy be appropriate for my symptoms?"
"Could low testosterone or high SHBG be contributing to my fatigue and low libido?"
"Can we retest in a few months if my symptoms persist, but labs were normal?"
When to consider retesting: If symptoms persist despite "normal" labs, consider repeating tests 2-3 months later. Hormonal variability means a single snapshot may not capture your pattern. If you're tracking your cycles, share that information—the relationship between cycle patterns and labs tells a story.
Remember: Clinical judgment matters more than any single lab value. A provider who listens to your symptoms, understands the nuances of perimenopausal physiology, and treats you rather than just your lab numbers is essential.

You Deserve to Be Heard
At Bonza Health, we believe that your experience is valid: even when your labs look "normal." The goal isn't to diagnose perimenopause (you likely already know something has changed). The goal is to understand your specific hormonal picture so we can tailor treatment to help you feel like yourself again.
Whether that means progesterone to help you sleep, cyclic estrogen to ease vasomotor symptoms, testosterone to restore your energy and libido, or simply a conversation with someone who understands that this transition is real: you have options.

Ready to have a different kind of conversation about your hormones? Book a consultation at bonzahealth.com, and let's create a personalized plan that honors both the science and your lived experience.
References:
[1] NICE, "Menopause: diagnosis and management," NICE Guideline NG23 (Updated 2024). Available: https://www.nice.org.uk/guidance/ng23
[2] S.D. Harlow et al., "Executive summary of the Stages of Reproductive Aging Workshop + 10," Fertil. Steril., vol. 97, no. 4, pp. 843-851, 2012. DOI: 10.1016/j.fertnstert.2012.01.128
[3] S.M. Nelson et al., "Anti-Müllerian hormone for the diagnosis and prediction of menopause: a systematic review," Hum. Reprod. Update, vol. 29, no. 3, pp. 327-346, 2023. DOI: 10.1093/humupd/dmac045
[4] E.W. Freeman et al., "Anti-Mullerian hormone as a predictor of time to menopause," J. Clin. Endocrinol. Metab., vol. 97, no. 5, pp. 1673-1680, 2012. DOI: 10.1210/jc.2011-3032
[5] J.S. Finkelstein et al., "Antimullerian Hormone and Impending Menopause in Late Reproductive Age," J. Clin. Endocrinol. Metab., vol. 105, no. 4, 2020. DOI: 10.1210/clinem/dgz283
[6] M.R. Soules et al., "Executive summary: Stages of Reproductive Aging Workshop (STRAW)," Fertil. Steril., vol. 76, no. 5, pp. 874-878, 2001. DOI: 10.1016/S0015-0282(01)02909-0
[7] StatPearls, "Menopause," NCBI Bookshelf, NBK507826, Updated Dec. 2023. https://www.ncbi.nlm.nih.gov/books/NBK507826/
[8] J.C. Prior, "Progesterone for Symptomatic Perimenopause Treatment," Facts Views Vis. Obgyn., vol. 3, no. 2, pp. 109-120, 2011. PMCID: PMC3987489
[9] ASRM, "Current clinical irrelevance of luteal phase deficiency: a committee opinion," Fertil. Steril., 2015. https://www.reproductivefacts.org
[10] L. Newson, "The importance of testosterone for women," DrLouiseNewson.co.uk, 2024. https://www.drlouisenewson.co.uk/knowledge/the-importance-of-testosterone-for-women
[11] S.R. Davis et al., "Global Consensus Position Statement on the Use of Testosterone Therapy for Women," J. Clin. Endocrinol. Metab., vol. 104, no. 10, pp. 4660-4666, 2019. DOI: 10.1210/jc.2019-01603
[12] L. Newson, "Should we be prescribing testosterone to perimenopausal and menopausal women?," BJGP, 2020. PMCID: PMC7098532
[13] M.K. Sheridan et al., "Effect of transdermal testosterone therapy on mood and cognitive symptoms in peri- and postmenopausal women," Arch. Womens Ment. Health, 2024. DOI: 10.1007/s00737-024-01513-6
[14] S.J. Parish et al., "ISSWSH Clinical Practice Guideline for the Use of Systemic Testosterone for Hypoactive Sexual Desire in Women," J. Sex. Med., 2021. DOI: 10.1016/j.jsxm.2021.07.005
[15] C. Selby, "Sex hormone binding globulin: origin, function and clinical significance," Ann. Clin. Biochem., vol. 27, pp. 532-541, 1990. PubMed
[16] L. Ferrucci et al., "Sex hormone binding globulin levels across the adult lifespan in women," J. Clin. Endocrinol. Metab., 2006. PMCID: PMC2648802
[17] M.M. Hedderson et al., "Longitudinal changes in sex hormone binding globulin (SHBG) and risk of incident diabetes: the SWAN study," Diabetes Care, vol. 47, no. 4, pp. 676-683, 2024. DOI: 10.2337/dc23-1630
[18] S.N. Dolitsky et al., "Efficacy of progestin-only treatment for menopausal symptoms," Menopause, vol. 28, no. 2, pp. 217-224, 2021. DOI: 10.1097/GME.0000000000001676
[19] J.C. Prior et al., "Oral micronized progesterone for perimenopausal VMS: Phase III Canada-wide RCT," Sci. Rep., vol. 13, 9082, 2023. DOI: 10.1038/s41598-023-35826-w
[20] P.A. Regidor, "Progesterone in peri- and postmenopause: a review," Geburtshilfe Frauenheilkd., vol. 74, no. 11, pp. 995-1002, 2014. DOI: 10.1055/s-0034-1383297
[21] N. Panay et al., "Menopause and MHT in 2024: IMS White Paper," Climacteric, 2024. DOI: 10.1080/13697137.2024.2394950
[22] S. Mukherjee et al., "Update on Menopause Hormone Therapy; Current Indications," Clin. Endocrinol., 2025. DOI: 10.1111/cen.15211